ABSTRACT
OBJECTIVES: to analyze the prevalence of vitamin D deficiency and insufficiency among adolescents in northern Minas Gerais, identifying associated factors.
METHODS: cross-sectional study, with a sample by clusters of adolescents, probabilistic allocation, according to school, sex and age, in 2016. Sociodemographic and anthropometric characteristics, lifestyle and dietary habits, morbidities, use of medications and cardiovascular risk factors were evaluated. Vitamin D deficiency was defined as values ≤20 ng/mL, insufficiency as values >20 and <30 ng/mL and sufficiency as values ≥30 ng/mL. Hypovitaminosis D (deficiency and insufficiency) was defined as values ≤30 ng/mL. Associated factors were identified from Poisson regression, with a robust estimator, with definition of Prevalence Ratios and 95% Confidence Intervals.
RESULTS: 494 adolescents were evaluated; 57.0% had hypovitaminosis D. Factors associated with deficiency were age (p<0.001) and chronic respiratory disease (p=0.046), and factors associated with hypovitaminosis D were age (p=0.019) and increased body mass index (p=0.007). No biochemical variable related to cardiovascular risk remained in the final model.
CONCLUSION: high and worrying values of hypovitaminosis D were recorded among adolescents, especially among the youngest, with chronic respiratory disease and overweight.
Keywords:
Vitamin D, Vitamin D deficiency, Adolescent, Risk factors
RESUMO
OBJETIVOS: analisar a prevalência de deficiência e insuficiência de vitamina D entre adolescentes no norte de Minas Gerais, identificando fatores associados.
MÉTODOS: estudo transversal, com amostra por conglomerados de adolescentes, alocação probabilística, segundo escola, sexo e idade, em 2016. Foram avaliadas características sociodemográficas, antropométricas, hábitos de vida e alimentares, morbidades, uso de medicamentos e fatores de risco cardiovascular. Definiu-se deficiência de vitamina D para valores ≤20 ng/mL, insuficiência para valores >20 e <30 ng/mL e suficiência para valores ≥ 30 ng/mL. A hipovitaminose D (deficiência e insuficiência), foi definida para valores ≤30ng/mL. Os fatores associados foram identificados a partir da regressão de Poisson, com estimador robusto, com definição das Razões de Prevalência e Intervalos de Confiança de 95%.
RESULTADOS: foram avaliados 494 adolescentes; 57,0% apresentaram hipovitaminose D. Os fatores associados à deficiência foram a idade (p<0,001) e doença respiratória crônica (p=0,046) e os fatores associados à hipovitaminose D foram a idade (p=0,019) e o aumento no índice de massa corporal (p=0,007). Nenhuma variável bioquímica relacionada ao risco cardiovascular se manteve no modelo final.
CONCLUSÃO: foram registrados valores elevados e preocupantes de hipovitaminose D entre adolescentes, especialmente entre os mais jovens, com doença respiratória crônica e com excesso de peso.
Palavras-chave:
Vitamina D, Deficiência de vitamina D, Adolescente, Fatores de risco
IntroductionVitamin D is a steroid hormone that has an essential role in bone metabolism by means of its action in specific receptors present in tissues necessary for calcium homeostasis. Nevertheless, in the last decades, the literature has been registering additional biological actions of vitamin D, evidencing actions in the cardiovascular, endocrine, nervous, immune and respiratory system, among others.
1 Studies demonstrated that hypovitaminosis D stands out as a global public health problem that affect all age groups.
2-5Notwithstanding, it is important to consider that, due to the need for a higher supply of nutrients for adequate growth and development, children and adolescents are particularly vulnerable to low vitamin D levels, yet there is no routine guideline for its supplementation. The conclusion of bone growth demands adequate production of thyroid hormones, growth hormone, growth factor and sex steroids, however during the growth spurt in adolescence, the process of maturation of epiphysis and the bone mineral fixation depends substantially on sex steroids and vitamin D.
6In spite of vitamin D is mostly produced due to the action of ultraviolet B radiation over the skin, even in researches carried out in sunny regions of several countries, we observe an elevated prevalence of low levels of this vitamin, reinforcing the affirmative of it is a pandemic.
2,4,7,8 There are other already known factors that may influence on vitamin D levels, such as, for example, obesity, intestine malabsorption syndrome, skin pigmentation, nephrotic syndrome, use of some medications, among others.
9In Brazil, studies that approach the subject of vitamin D in children and adolescents are scarce. A geospatial meta-analysis in Brazil concerning vitamin D insufficiency and deficiency reported the prevalence of deficiency and insufficiency of vitamin D of 28.16% and 45.26%, respectively. The highest prevalence of vitamin D deficiency was observed in the South and Southeast regions, and the highest occurrence of insufficiency was observed in the Southeast and Northeast regions. In the mentioned analysis, only 15.7% of studies included the adolescent age group and none of them was performed in the North of Minas Gerais. The authors alert for the need for opportune interventions, considering the high prevalence of inadequate concentrations of vitamin D, independently of the age range.
7The Survey of Cardiovascular Risks in Adolescents (ERICA – Portuguese acronym), a Brazilian survey with adolescents from 12 to 17 years of age that assessed vitamin D levels and associated factors in four capitals from different regions, found a prevalence of deficiency and insufficiency of vitamin D of 21% and 42%, respectively, evidencing high prevalence of risk of hypovitaminosis D for Brazilian adolescents, regardless of the region.
5For the North of Minas Gerais, a transition area between the Southeast and Northeast of Brazil, with high solar irradiation indexes, there are no studies on vitamin D levels in adolescents. The aim of this research was to analyze the prevalence of deficiency and insufficiency of vitamin D within adolescents in the North of Minas Gerais, identifying associated factors.
MethodsCross-sectional analytic study nested within an interventional study, which assessed the influence of a physical activity program for adolescents. The population of the present study was composed of students of both sexes, regularly enrolled in elementary school and high school of the public network of the city of Montes Claros (MG). The city is the main urban center of the region, located in latitude -16.737 and longitude -43.8647, with a population of approximately 415 thousand inhabitants and is a reference in the provision of health services for neighboring municipalities.
The target population of the study was composed of teenage students from public schools of the municipality. The sample selection occurred by means of clusters, with probabilistic allocation of schools and grades, through the spatial distribution of the schools in the municipality. The process occurred in two stages, using cluster sampling. In the first stage, the population enrolled was extracted from four areas of the city. Posteriorly, we identified the number of public schools and the number of students enrolled per area. In the second stage, the sampling weights as inverse probability weighting for the inclusion of each area were calculated and measured according to the number of students enrolled in the schools. In sequence, there was the selection of adolescents, with systematic random sampling, with substitutions when necessary. The representativeness of the population was considered having the reference for this proportionality the number of students according to sex and age. The sample size was established to estimate population parameters considering an estimated prevalence of 50%, which assures higher sample size. We established a 95% confidence level and a 5% margin of error. We performed the finite population correction and design effect correction, considering a factor of 1.5.
Were eligible for the study adolescents of both genders, aged from ten to 18 years, regularly enrolled in the selected schools. We excluded adolescents that self-reported having significant kidney disease, inflammatory, infectious hepatic or hematological diseases, besides those using medications that influenced the metabolic and/or hemodynamic profile and pregnant girls.
Data collection occurred in the beginning of the second semester of school, between August and October 2016, in the end of the summer and onset of spring, a period in which the season does not impair outdoor activities.The team of collection was specifically trained and was composed of physicians, physical education professionals and scientific initiation students. The adolescents were guided about the 12 hours fasting before the collection.
We used semi-structured questionnaires, approaching demographic and socioeconomic variables, use of medications, morbidities, eating habits and life habits. The variables applied were defined by the researchers based on similar studies. For information on food consumption, we used items of the food records. The registry of use of medications and morbidities, including chronic respiratory disease, was measured from the report of adolescents. The questionnaire was fulfilled by the adolescents themselves, under guidance of researchers.
We performed anthropometric measures of weight and height for the calculation of body mass index (BMI), besides the abdominal circumference, considering as reference the WHO guidelines, and following the specific protocols for each measurement.
10 The cutoff points for BMI were defined from the z score, in the following manner: score z ≥ -2 e ≤ 1: normal, score z > 1 and ≤ 2: overweight and score z > 2: obesity. For statistical analysis, BMI was categorized into normal and weight excess (overweight and obesity). Central obesity was considered by means of the measure of the waist circumference (WC) and the values were considered high when WC ≥ percentile 90.
11 We measured blood pressure (BP), which was considered high, according to criteria from the International Diabetes Federation (IDF), when BP> percentile 95 for sex, age and height or when Systolic Blood Pressure ≥130mmHg or Diastolic Blood Pressure ≥85mmHg.
11,12Biochemical markers and of cardiovascular risk, besides vitamin D, were assessed by means of blood samples collected in the school, with venipuncture performed by specialized mid-level practitioners, with disposable needles and syringes. The biochemical tests of glucose (GLU), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG) were performed using enzymatic methods with automatized equipment. For hyperglycemia, the cutoff point considered was GLU≥100 mg/dl.
11 The low-density lipoprotein cholesterol (LDL-C) was calculated with Friedewald formula. The non-HDL cholesterol was calculated with the formula TC – HDL-c. Dyslipidemia was defined by the presence of at least one of the following parameters: TC ≥ 170 mg/dL, HDL-c ≥ 45 mg/dL, LDL-c ≥ 110mg/dL, non-HDL cholesterol ≥ 120 mg/dL or TG ≥90mg/dL.
13Metabolic syndrome was diagnosed in participants according to criteria proposed by IDF: (1) central obesity (WC ≥ 90 percentile for those with ten to 15 years or WC 90 cm for men and 80 cm for women in those aged 16 years); (2) SBP ≥130 or DBP ≥85 mmHg; (3) TG ≥ 150 mg/dL; (4) HDL-C ≥ 45 mg/dL for those with ten to 15 years, HDL-C ≥45 mg/dL in men and ≥40 mg/dL in women for those with 16 and 17 years; (5) fasting glycaemia GLU ≥ 100 mg/dL.
11,12 Participants with central obesity and any two more of the other four factors were considered as having metabolic syndrome.
Insulin (INS) and vitamin D (VitD) were measured using chemiluminescent immunoassay. We considered hyperinsulinemia values of INS ≥ 20 mU/L and insulin resistance (IR) with values calculated of HOMA-IR ≥ 3.16.
14,15 For the 25-hydroxyvitamin D (25-OH vitamin D), the cutoff values for each variation group were: deficiency for values ≥20 ng/mL; insufficiency for values >20 and <30 ng/mL and sufficiency when values ≥ 30ng/ml. It is important to highlight that these values are the same recommended for adults and used in similar studies.
2,3,5-7We did not perform the Tanner staging for pubertal development, considering the logistical difficulty in the assessment and ethic-law aspects for the procedure, because the collection sites did not have private rooms.
The variables were analyzed with the statistical software SPSS (Statistical Program for Social Sciences) version 20.0 for Windows. After descriptive analysis, we performed bivariate analyses (Pearson’s chi-square test or Fisher’s exact test) and the variables that presented significance levels of up to 20% (
p<0.20) were assessed jointly with Poisson regression, with robust estimators. For the final model, we estimated prevalence ratios and the respective 95% confidence intervals, assuming a significance level of 5% (
p<0.05).
The project of this study was submitted to the Research Ethics Committee of the State University of Montes Claros (Unimontes – Portuguese acronym) and was approved with opinion number 1.503.680.
ResultsA total of 494 students participated in the study, 296 (59.9%) were female and 373 (75.8%) self-declared as being black (brown or black skin color). Most of the assessed group (85.6%) informed a family income of up to three minimum wages. These and other group characteristics are demonstrated in Tables 1 and 2. The vitamin D levels assessed revealed that 67 (13.8%) adolescents had deficiency of the vitamin, 209 (43.2%) presented insufficient levels and 208 (43.0%) had values considered sufficient.
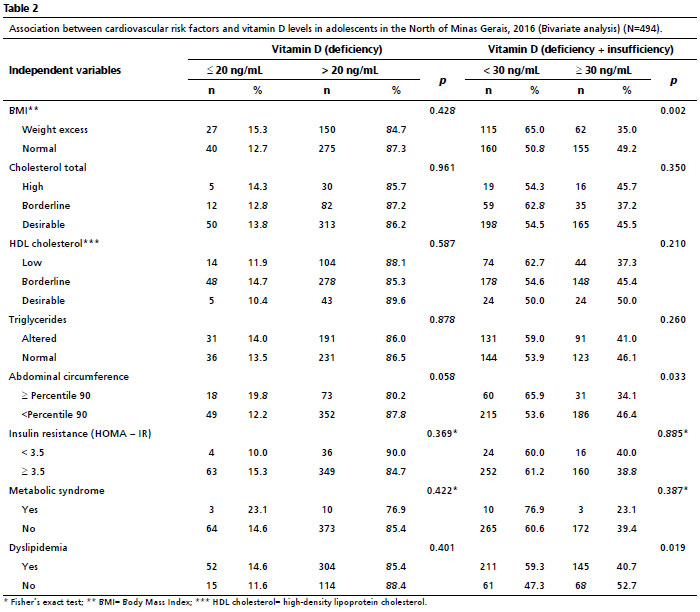
Table 1 presents results of the bivariate analysis in relation to sociodemographic characteristics and life habits for the values of vitamin D deficiency and of hypovitaminosis D (deficiency+insufficiency). Table 2 presents results of the bivariate analysis related to anthropometric and biological parameters considered cardiovascular risk factors.
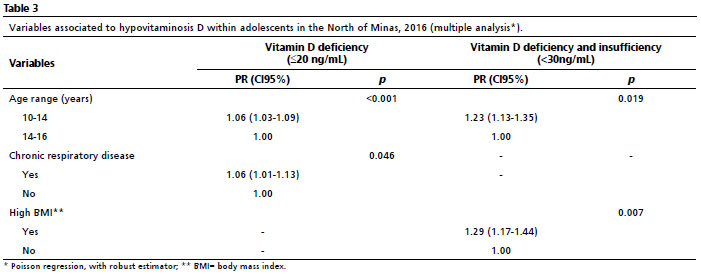
Table 3 presents the result of the multiple analysis considering all factors associated until the 20% level of the bivariate analysis. The age group from 10 to 14 years was a factor associated with both vitamin D deficiency and hypovitaminosis D (deficiency + insufficiency). The registry of chronic respiratory disease was also associated with vitamin D deficiency, and high BMI was associated with higher prevalence of hypovitaminosis D.
DiscussionThis study assessed vitamin D levels in adolescents from public schools in the North of Minas Gerais, an area of high solar irradiation indexes, revealing an important prevalence of deficiency and insufficiency of this vitamin. Hilger
et al.
2 demonstrate, in a systematic review about vitamin D status in the world population, a scarcity of studies of this nature in South America, with only one from Argentina and two from Brazil. Specifically in Brazil, a study of geospatial meta-analysis highlighted high prevalence of deficiency and insufficiency of vitamin D in the general population.
7Two other global systematic reviews published in 2013 and 2016 demonstrate increased prevalence for both deficiency and insufficiency of vitamin D, reinforcing the affirmative that this is a worldwide problem of public health.
4,16 The meta-analysis carried out by Palacios and Gonzalez,
16 specially, assessed risk groups for this issue and indicates adolescents as one of the risk groups to be monitored. Assessing only studies concerning prevalence of representative samples, the authors concluded that the occurrence of low levels of vitamin D is a worldwide problem in all age groups, even highlighting an impressive lack of data for children and adolescents in the entire world.
16For the ERICA study, authors observed also in Brazil a high prevalence of deficiency and insufficiency of the vitamin for the adolescent population, regardless of the region assessed. Hypovitaminosis D was positively associated with female sex, with latitudes, with the period of data collection, skin color (non-white) and students from private schools. It is important to register that the present study presented a correspondence of the hypovitaminosis D levels investigated in the ERICA survey, reiterating the critical situation of low vitamin D levels.
5A national research, carried out from a large sample of laboratory data observed that the adolescent age range have a percentage of individuals with vitamin D <20 ng/mL with values of 13.4% and 12.6% in the male and female genders, respectively, which indicates an increase of over two times compared with the infant age range.
17 The present study does not allow the comparison by age ranges throughout life, although the prevalence for the same vitamin D levels in these adolescents are similar and expose a severe impairment for this risk group. Highlighting the magnitude of the problem in Australian adolescents, a study registered a slightly higher prevalence than that observed in this study for vitamin D deficiency, of 17.0% and even higher for hypovitaminosis D, of 65.0%.
18In a more recent meta-analysis, the authors gathered 308 studies that investigate the prevalence of vitamin D deficiency in population based analyses from 2020 to 2022, in 81 countries. Worldwide, they registered levels of deficiency and insufficiency at 15.7% and 47.9% of the population, respectively. The authors highlight that the values are concerning, considering that low vitamin D values would increase the global load of diseases and that the governments should consider its prevention as a public health priority.
19There is a significant divergence in the literature about risk factors for hypovitaminosis D, which involves environmental aspects, biological and demographic characteristics, eating habits, among others.
4,5,8,19-21 In this study, the assessed variables sex, skin color, family income, physical activity, regular use of sunscreen and an adequate consumption of meat, eggs, milk and dairy products were not associated to low vitamin D levels. It is possible that at least part of this divergence observed is due to the uniformity of the participants in the study, since all of them were from public schools and present very similar socioeconomic conditions.
The results registered association between low vitamin D levels and age range, with predominance in the early adolescence stage (adolescents between ten and 14 years) for both deficiency and hypovitaminosis D. It is not a variable systematically assessed in other studies. Nevertheless, another national study, in a sunny region of Brazilian Northeast, however it was carried out with overweight adolescents, presented the same behavior in relation to age range observed in this study, demonstrating progressive improvement of hypovitaminosis D prevalence as the adolescents got older.
22 The meta-analysis of Hilger
et al.,
2 which compared variations of the levels of vitamin D worldwide and assessed differences by age, sex and geographic region did not find differences related to age.
2Another factor associated with low vitamin D levels in the present study was the report of chronic respiratory disease in adolescents. In a revision about the extraskeletal effects of vitamin D, the authors highlighted the effects of this micronutrient in the modulation of the function of B and T lymphocytes, and their impact in inflammatory pathways, and relate the deficiency of the vitamin with increased risk of respiratory infections, worsening of pulmonary function, exacerbation of asthma and worsening of prognosis of patients with asthma.
23,24 In China, researchers reinforced these observations and explain that the active form of the vitamin performs its physiological effects when linked to specific receptors that are broadly distributed within epithelial respiratory cells and immune cells (B cells, T cells, macrophages and monocytes). These receptors regulate the transcription of several genes related to immunomodulation and inflammation.
24Hypovitaminosis D has been related to metabolism deviations, specifically the metabolism of carbohydrates and metabolic syndrome (MS). In this study, no biochemical marker of cardiovascular risk was associated to hypovitaminosis D. In a revision about the extraskeletal effects of vitamin D, the authors presented several studies that confirmed the association between low levels of this vitamin with Diabetes Mellitus and MS, however they also shown some studies with conflicting results.
25 Effectively, the role of vitamin D deficiency in several extraskeletal diseases, in the molecular perspective, particularly in relation to metabolic syndrome, still lacks better comprehension and new studies.
The BMI when in values consistent with obesity and overweight, in this study considered jointly as weight excess, was associated with hypovitaminosis D but did not present a statistically significant association with vitamin D deficiency. A Brazilian study that assessed the association between cardio-metabolic risk factors and hypovitaminosis D in the Northeast of Brazil assessed 125 adolescents, registering a frequency of hypovitaminosis D of 45.6%. The variables that were associated to hypovitaminosis were blood pressure above the 95 percentile, body weight and fasting insulin.
22 The results are consistent with the present study only with regard to weight excess, nevertheless it is relevant to highlight that the number of the abovementioned study was significantly lower and based in a convenience sample.
Another Brazilian study using a slightly higher adolescent age range (from 15 to 19 years) also find high prevalence of hypovitaminosis D, of 57.3% in the study population as a factor independently associated with weight excess only for the male gender.
26 An international survey for the definition of standards for overweight and obesity within children and adolescents in the world, in which the Brazilian infant population was also assessed, demonstrated that there is a peak in the coefficient of BMI variation in puberty for both sexes.
27 Being puberty the age range of this study, this evidence reinforces the hypothesis that the lower bioavailability of vitamin D observed in individuals with obesity may be attributed, among other factors, to the sequestration of vitamin D in the adipose tissue.
22,28 The results of studies already performed present evidence that suggests that, besides obesity is related to vitamin D storage in adipocytes leading to the reduction of its bioavailability, the adipose tissue present lower expression of enzymes responsible for the hydroxylation of vitamin D, as well as specifically 1-α-hydroxylase, which may impair its activities in obesity.
26Concerning other cardiovascular risk factors, the biochemical and metabolic variables, which include the calculation of HOMA index and/or the diagnosis of metabolic syndrome, were not statistically associated with hypovitaminosis D (deficiency and/or insufficiency) in this research as well. This is still an unclear relationship in the literature, with studies that present conflicting results. In an Australian study started in 1989 and published in 2016, the authors investigated, in adolescents and young adults, the prospective associations between serum concentrations of vitamin D and risk factors, such as BMI, insulin resistance, HDL-cholesterol, triglycerides and systolic arterial pressure, evidencing that serum concentrations of vitamin D were inversely associated to BMI and insulin resistance, suggesting a cardio-protective benefit in the increase of vitamin D levels.
29On the other hand, a study carried out in China with 2680 children and adolescents revealed that low vitamin D levels were associated to obesity, however it did not occur to any other cardiovascular risk factor.
30 Also in other studies carried out in Brazil, the authors did not observe association between dyslipidemia or insulin resistance and vitamin D levels.
22,26 Yet other cardiovascular risk factors did not show association with vitamin D in this study, the presence of statistical significance of the latter with BMI increase, itself, deserves attention and a better understanding of the subject since high BMI in children and adolescent are directly related to the increase of coronary disease in adulthood.
The results of this study should be considered in the light of some limitations. The study group is relatively homogeneous in relation to socioeconomic characteristics, considering that all of them were allocated from public schools. Various information concerning the subject, such as physical activity, diet, among others, were registered from the reports of adolescents, without the help of more validated or accurate instruments or measures of control. In this perspective, also, we highlight that no direct measurement of the time of sun exposure was registered, as well as the use of clothes and/or accessories of sun protection. In addition, the collection of blood samples was performed in the same period of year, in spite of the absence or well-defined seasons in the region, which may justify behaviors of less or more sun exposure in outdoor environments. Finally, it is important to mention that, although the cutoff points used are the same as those of other studies, these values are also used for adults, being possible that adolescents have different concentrations of vitamin D.
In spite of these limitations, considering the scarcity of regional studies, the results are relevant since they expose a critical condition, which was unknown for the region, for a population group particularly more vulnerable, that is, adolescents from public schools. The results generated will serve to base other studies and to the guidance of managers and health professionals in the definition of public health policies and approaches in the change of habits in this population.
The present study assessed simultaneously factors associated with both vitamin D deficiency and hypovitaminosis D (deficiency + insufficiency), registering that chronic respiratory disease was associated to deficiency, but not to hypovitaminosis D, whilst the increase of body mass index was associated to hypovitaminosis D, but not to deficiency. This result emphasizes that the actions of vitamin D for beyond the skeletal system still lack further studies. On the other hand, the need for standardization of serum levels for vitamin D for the assessed group still occurs, for both the clinical perspective and epidemiological studies.
References1. Rebelos E, Tentolouris N, Jude E. The Role of Vitamin D in Health and Disease: A Narrative Review on the Mechanisms Linking Vitamin D with Disease and the Effects of Supplementation. Drugs. 2023; 83 (8): 665-85.
2. Hilger J, Friedel A, Herr R, Rausch T, Roos F, Wahl DA,
et al. A systematic review of vitamin D status in populations worldwide. Br J Nutr. 2014; 111 (1): 23-45.
3. Basatemur E, Horsfall L, Marston L, Rait G, Sutcliffe A. Trends in the Diagnosis of Vitamin D Deficiency. Pediatrics. 2017; 139 (3): e20162748.
4. Cashman KD, Dowling KG, Škrabáková Z, Gonzalez-Gross M, Valtueña J, De Henauw S,
et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016; 103 (4): 1033-44.
5. Oliveira CL, Cureau FV, Cople-Rodrigues CDS, Giannini DT, Bloch KV, Kuschnir MCC,
et al. Prevalence and factors associated with hypovitaminosis D in adolescents from a sunny country: Findings from the ERICA survey. J Steroid Biochem Mol Biol. 2020; 199: 105609.
6. Taylor SN. Vitamin D in Toddlers, Preschool Children, and Adolescents. Ann Nutr Metab. 2020; 76 (Suppl. 2): 30-41.
7. Pereira-Santos M, Santos JYGD, Carvalho GQ, Santos DBD, Oliveira AM. Epidemiology of vitamin D insufficiency and deficiency in a population in a sunny country: Geospatial meta-analysis in Brazil. Crit Rev Food Sci Nutr. 2019; 59 (13): 2102-9.
8. Rutigliano I, De Filippo G, De Giovanni D, Campanozzi A. Is sunlight enough for sufficient vitamin D status in children and adolescents? A survey in a sunny region of southern Italy. Nutr. 2021; 84: 111101.
9. Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP,
et al.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011; 96 (7): 1911-30.
10. Onis M, Onyango AW, Borghi E, Siyam A, Nishida C,
et al. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007; 85 (9): 660-7.
11. Zimmet P, Alberti KG, Kaufman F, Tajima N, Silink M, Arslanian S,
et al.; IDF Consensus Group. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr Diabetes. 2007; 8 (5): 299-306.
12. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004; 114 (2 Suppl. 4
th Report): 555-76.
13. Faludi AA, Izar MCO, Saraiva JFK, Chacra APM, Bianco HT, Afiune A Neto,
et al. Atualização da Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose – 2017. Arq Bras Cardiol. 2017; 109 (2 Supl. 1): 1-76.
14. Bloch KV, Szklo M, Kuschnir MC, Abreu GA, Barufaldi LA, Klein CH,
et al. The Study of Cardiovascular Risk in Adolescents--ERICA: rationale, design and sample characteristics of a national survey examining cardiovascular risk factor profile in Brazilian adolescents. BMC Public Health. 2015; 15: 94.
15. Keskin M, Kurtoglu S, Kendirci M, Atabek ME, Yazici C. Homeostasis model assessment is more reliable than the fasting glucose/ insulin ratio and quantitative insulin sensitivity check index for assessing insulin resistance among obese children and adolescents. Pediatrics. 2005; 115 (4): 500-3.
16. Palacios C, Gonzalez L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol. 2014; 144 (Pt A): 138-45.
17. Leão LMCSM, Rodrigues BC, Dias PTP, Gehrke B, Souza TDSP, Hirose CK,
et al. Vitamin D status and prevalence of hypovitaminosis D in different genders throughout life stages: A Brazilian cross-sectional study. Clinics (Sao Paulo). 2021; 76: e2571.
18. Horton-French K, Dunlop E, Lucas RM, Pereira G, Black LJ
. Prevalence and predictors of vitamin D deficiency in a nationally representative sample of Australian adolescents and young adults. Eur J Clin Nutr. 2021; 75: 1627-36.
19. Cui A, Zhang T, Xiao P, Fan Z, Wang H, Zhuang Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front Nutr. 2023; 10: 1070808.
20. Hu Y, Chen J, Wang R, Li M, Yun C, Li W,
et al. Vitamin D Nutritional Status and its Related Factors for Chinese Children and Adolescents in 2010-2012. Nutrients. 2017; 9 (9): 1024.
21. Haq A, Svobodová J, Sofi NY, Jindrová A, Kába B, Rajah J,
et al. Vitamin D status among the juvenile population: a retrospective study. J Steroid Biochem Mol Biol. 2018; 175: 49-54.
22. Souza ALS, Araújo EPDS, Souza TO, Pimentel JB, Ferreira ALM, David DFOS,
et al. Cardiometabolic risk factors and hypovitaminosis D in adolescents with overweight from a sunny region in northeast Brazil: a cross-sectional study. Nutr Hosp. 2022; 39 (1): 73-81.
23. Marino R, Misra M. Extra-Skeletal Effects of Vitamin D. Nutrients. 2019; 11 (7): 1460.
24. Liu J, Dong YQ, Yin J, Yao J, Shen J, Sheng GJ,
et al. Meta-analysis of vitamin D and lung function in patients with asthma. Respir Res. 2019; 20 (1): 161.
25. Zendehdel A, Arefi M. Molecular evidence of role of vitamin D deficiency in various extraskeletal diseases. J Cell Biochem. 2019; 120 (6): 8829-40.
26. Araújo EPS, Queiroz DJM, Neves JPR, Lacerda LM, Gonçalves MDCR, Carvalho AT. Prevalence of hypovitaminosis D and associated factors in adolescent students of a capital of northeastern Brazil. Nutr Hosp. 2017; 34 (5): 1416-23.
27. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000; 320(7244):1240-3.
28. Vanlint S. Vitamin D and obesity. Nutrients. 2013; 5 (3): 949-56.
29. Black LJ, Burrows S, Lucas RM, Marshall CE, Huang RC, Chan She Ping-Delfos W,
et al. Serum 25-hydroxyvitamin D concentrations and cardiometabolic risk factors in adolescents and young adults. Br J Nutr. 2016; 115 (11): 1994-2002.
30. Tang Z, Huang S, Ma R, Zheng H, Zhu Y. Low vitamin D status is associated with obesity but no other cardiovascular risk factors in Chinese children and adolescents. Nutr Metab Cardiovasc Dis. 2020; 30 (9): 1573-81.
Authors’ contributionDavid GG:project elaboration, data analysis and collection, elaboration and review of the manuscript. Maia JEF and Freitas OCS: data analysis, support to literature review, elaboration and writing of the manuscript. Caldeira AP: project elaboration, data analysis, literature review and elaboration, general coordination of the research. All authors approved the final version of the article and declare no conflicts of interest.
Received on January 27, 2024
Final version presented on August 21, 2024
Approved on August 23 2024
Associated Editor: Pricila Mullachery


 ; Jeniffer Elisa Ferreira Maia 2
; Jeniffer Elisa Ferreira Maia 2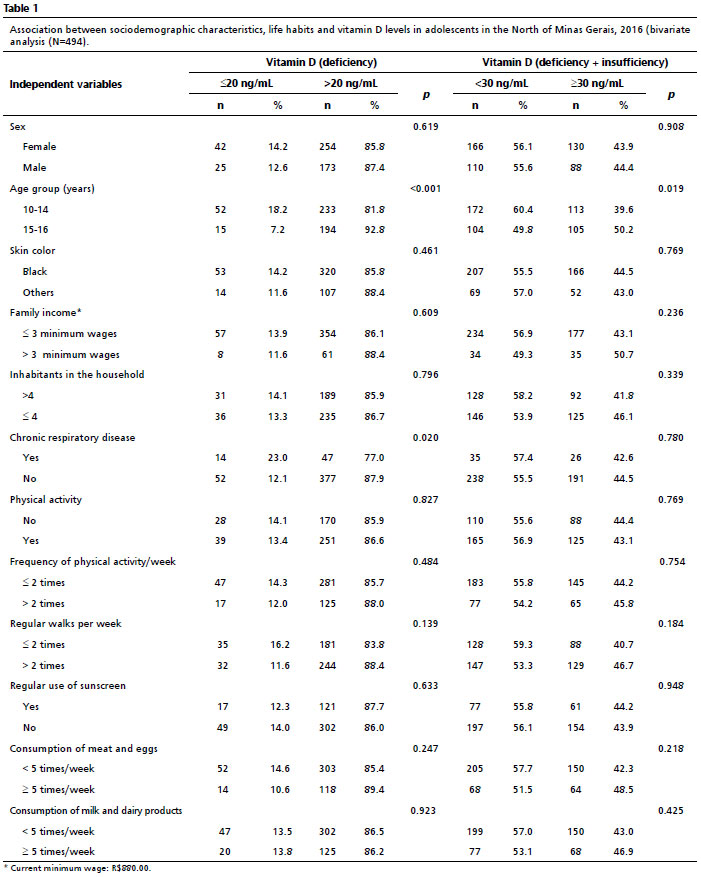






 Ler em português
Ler em português