ABSTRACT
OBJECTIVES: to identify dietary patterns (DP) of postpartum women and to evaluate the effect of food insecurity, age, and level of schooling on unhealthy DP.
METHODS: Cohort carried out by non-probabilistic consecutive sampling process in a city in the Northeast region in Brazil, between 2017-2018. From the food frequency questionnaires, DP were derived by principal component analysis in the 3rd (n=207), 6th (n=195), and 12th month (n=183) postpartum. The associations between DP and the independent variables were investigated using mixed effects logistic regression model.
RESULTS: two dietary patterns were identified: predominantly healthy DP (PHDP) and predominantly ultra-processed DP (PUPDP). It was found that the higher the age (OR= 0.92; CI95%= 0.85-0.99; p=0.031) and the level of schooling (OR= 0.81; CI95%= 0.70-0.93; p=0.003), the lower the chance of adherence to PUPDP. Families with some level of food insecurity were more likely to adhere to PUPDP (OR= 1.55; CI95%= 1.01-2.37; p=0.044).
CONCLUSION: adherence to PUPDP increases with the level of food insecurity. The higher age and level of schooling decrease adherence to this DP. These findings provide support for the association between food insecurity, age and education with adherence to PUPDP, suggesting the need for effective measures to ensure food security, particularly for vulnerable populations.
Keywords:
Dietary patterns, Postpartum period, Food insecurity, Cohort studies
RESUMO
OBJETIVOS: identificar padrões alimentares (PA) de mulheres pós-parto e avaliar o efeito da insegurança alimentar, da idade e do nível de escolaridade no PA não saudável.
MÉTODOS: Coorte realizada por processo de amostragem consecutiva não probabilística em município da região Nordeste do Brasil, entre 2017-2018. A partir dos questionários de frequência alimentar, foram derivados PA por análises de componentes principais no 3º (n=207), 6º (n=195) e 12º mês (n=183) pós-parto. As associações entre os PA e as variáveis independentes foram investigadas utilizando modelo de regressão logística de efeitos mistos.
RESULTADOS: foram identificados dois padrões alimentares: PA predominantemente saudável (PAPS) e PA predominantemente ultraprocessado (PAPUP). Identificou-se que quanto maior a idade (OR= 0,92; IC95%= 0,85-0,99; p=0,031) e o nível de escolaridade (OR= 0,81; IC95%= 0,70-0,93; p=0,003), menor foi a chance de adesão ao PAPUP. Famílias com algum nível de insegurança alimentar apresentaram maior chance de aderir ao PAPUP (OR= 1,55; IC95%= 1,01-2,37; p=0,044).
CONCLUSÃO: a adesão ao PAPUP aumenta com o nível de insegurança alimentar. A maior idade e nível de escolaridade diminuem a adesão a esse PA. Esses achados fornecem suporte para a associação entre insegurança alimentar, idade e escolaridade com a adesão ao PAPUP, sugerindo a necessidade de medidas eficazes para garantir a segurança alimentar, particularmente para populações vulneráveis.
Palavras-chave:
Padrões alimentares, Período pós-parto, Insegurança alimentar, Estudos de coorte
IntroductionAn inadequate dietary intake predisposes to a greater risk of developing nutritional disorders, including micronutrient deficiencies, among other forms of malnutrition, especially among the most vulnerable population groups, such as women of reproductive age.
1The dietary guide for the Brazilian population recommends limiting the consumption of processed food and avoiding ultra-processed food, as a general rule.
2 This recommendation should apply even more strongly to women during pregnancy and the postpartum period.
2,3 At this stage of the life cycle it is essential for women to receive nutritional guidance for a healthy and adequate diet, considering that healthy behaviors are fundamental to women and children’s health.
1,3However, transformations in the global food system have led to changes in the dietary patterns (DP) of the Brazilian and global populations, including an increasing consumption of ultra-processed food and drinks.
4 Women tend to have healthier eating behaviors during pregnancy.
5 However, the quality of diet tends to decrease after giving birth, with an increase in the consumption of processed food and a reduction in the consumption of fruit and vegetables, especially in the first six months after giving birth.
5,6 Over the years, however, we have seen that the dietary intake of pregnant women, women who have recently given birth and puerperal women has consisted of DPs dominated by ultra-processed food.
7,8Women’s food consumption is influenced by several factors. According to the study, women with a lower level of schooling are more likely to adhere to less healthy DP, including ultra-processed food, while women with more years of schooling tend to adhere to healthier DPs.
9 Age is considered one of the factors that most determine adherence to DP.
10 In general, age can act as a protective factor for healthy eating, as studies show a trend towards lower consumption of ultra-processed food as you get older.
10,11The relation between food insecurity and the consumption of ultra-processed food has been the subject of interest in the scientific literature.
12 Studies indicate that food insecurity is associated with unhealthy DP adherence, particularly in economically more vulnerable populations.
12,13Food insecurity poses barriers to the adoption of a healthy diet, as it makes it difficult to access these food (physically/financially), favoring the consumption of unhealthy, cheap and accessible food. This situation is of particular concern among women of reproductive age, given the high nutritional demands at this stage of the life cycle.
13In view of the above and considering that diet is a modifiable component related to important maternal and neonatal outcomes, the aim of this study was to identify DPs of puerperal women with high socioeconomic vulnerability, and to analyze the effect of food insecurity, age and education on unhealthy DP.
MethodsThis study is a prospective cohort, developed in Rio Largo/Alagoas, which followed women and their conceptus during the first year postpartum. The city of Rio Largo is located in the State of Alagoas, in theNortheast region of Brazil, a strategic territory, due to its similar characteristics to the state that hosts it, such as sociodemographic and economic conditions, health determinants and the Human Development Index (HDI),
14 conferring external validity on the results, such others city in the Northeast region.
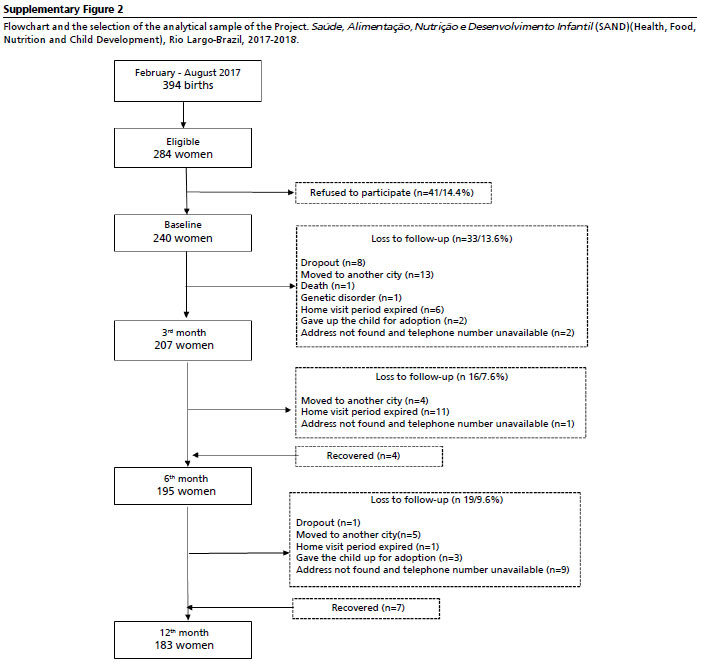
A non-probabilistic consecutive sampling process was carried out by convenience. The study included women who gave birth between February and August 2017 in the only public hospital in the city, which has a low-risk maternity. Women who did not live in the city and those with HIV/AIDS were excluded. Of the 284 eligible women, 240 were recruited.
Data collection occurred in four waves over 12 months: immediate postpartum (maternity), third, sixth and twelfth month postpartum by home visits. Supplementary Figure 1 shows the flowchart of study participants and losses to follow-up.
A semi-quantitative food frequency questionnaire (FFQ) validated for the Brazilian population was used to identify DPs.
15 The instrument contains 110 items, and includes the usual food consumed by the population studied. It was applied on the third (n=207), sixth (n=195) and twelfth (n=183) months postpartum. Data were collected by trained interviewers.
The FFQ was composed of nine categories of consumption frequency, with options of response ranging from ‘does not consume’ to ‘consumes more than three times/day’, later converted into the following score: “more than 3 times/day”=3; “2-3 times/day”=2; “1 time/day”=1; “5-6 times/week”=0.78; “2-4 times/week”=0.42; “1 time/week”=0.14; “1-3 times/month”=0.07; “hardly ever/never”=0.010; “seasonal consumption”=0.005. For the answer “does not consume”, was assigned a value=0.00.
The first application of the FFQ (three months postpartum) obtained data on the last year (pregnancy and the first three months postpartum). On the sixth and twelfth months, data were collected relating to the last quarter and last semester, respectively.
Food with a consumption frequency of less than 5% were excluded (e.g., soy extract, which had a participation rate of 1.5%). The group of rice, bread, corn-derived food and alcoholic beverages were not included in the analysis as they had a very low factorial load. The items were grouped into 11 food groups, based on nutritional similarity, in coherence with literature.
16 Table 1 shows the groups and their respective food that made up the DP with the highest adherence.
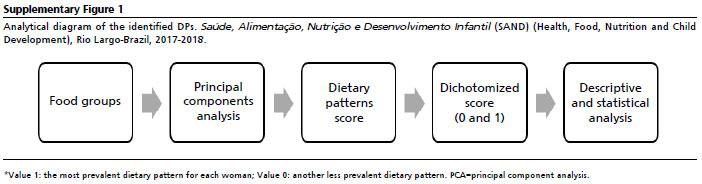
The DP shows standardized scores generated for each woman evaluated. For each DP identified, standardized scores were generated for each woman. It was assumed that the score value represented the women’s proximity to the DP and it was assigned to each woman the DP with the highest probability of adherence. Thus, in the model, dichotomous variables were generated and attributed a single DP to each individual, identifying the DP that best characterizes the individuals, as proposed in a previous study
17 (Supplementary Figure 1).
The perception of food insecurity was assessed using the
Escala Brasileira de Insegurança Alimentar (EBIA) (Brazilian Insecurity Scale), applied in the immediate postpartum, considering access to food in the last three months. Each affirmative answer on the questionnaire is equivalent to one point, and the sum of the points gives the total score on the scale; the classification is based on the sum of points, which ranges from zero to 15. The classification was carried out as follows: 0: security; 1-5: mild insecurity; 6-10: moderate insecurity; and 11-14: severe insecurity. Estimates were calculated based on using this variable at its four levels.
18Data on the immediate postpartum period were analyzed to characterize the population: age (<20 years and ≥20 years), as recommended by World Health Organization
19; years of study/schooling (≤8 years and >8 years); family’s economic class (Class B+C and Class D+E), assessed according to the
Critério de Classificação Econômica Brasil20 (Brazil Economic Classification Criteria), a household assets-based form that includes the head of the family’s educational level and availability of sanitation services and street pavement; and number of children (≤2 child >2 child). For the model, time variables (third, sixth and twelfth months postpartum), age in years and schooling (years of study) were used as continuous and food insecurity as ordinal variable, based on the score obtained, in four categories: food security/none insecurity; mild, moderate and severe food insecurity.
The data was double-entered/validated in Epi-Info3.5.4 [Centers for Disease Control/Prevention], Atlanta, USA). Statistical analyses were carried out using Stata/SE 13 (StataCorp LP, College Station, TX, USA).
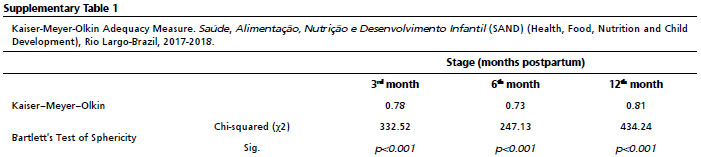
Descriptive statistics were used to compare the characteristics of the women included and excluded, using Fisher’s exact test. DPs were derived using principal component analysis (PCA), which reduces the number of variables based on the correlation of groups. The varimax rotation method was applied to simplify the interpretation of the extracted factors. The suitability of the data set for applying the PCA was confirmed by the Kaiser-Meyer-Olkin (KMO >0.50) and Bartlett ‘s test of sphericity (
p<0.05).
The number of factors was defined based on the components with an eigenvaluegreater than 1. Each principal component was interpreted based on food with factor loadings ≥0.3. The naming of the DPs was determined from the food that made up the components.
To examine the longitudinal association between DP, time, food insecurity, age and level of schooling we conducted mixed effects logistic regression model. Time, food insecurity, age and schooling were used as fixed effects. For the random effect, which allows for variation in the coefficients to be estimated, the individual (women) and time were included. This modeling has two components: intra-individual (longitudinal change described by model with a population-cluster intercept and slope) and between individuals (variation in the individual intercept and slope). The statistical strategy adopted allows for the analysis of temporally unbalanced measures, as well as missing information.
21 The unstructured covariance matrix was used for this model, considering the number of children and whether they breastfed at any stage of the study. These variables were inserted as model adjustment. For all the tests applied,
p≤0.05 to be statistically significant. Estimates were presented as odds ratio (OR) with their respective 95% confidence interval (CI95%).
The ResearchEthics Committee of
Universidade Federal de Alagoas approved the study protocol SAND (CAAE: 5483816.9.0000.5013), acronym for “
Saúde, Alimentação, Nutrição e Desenvolvimento Infantil” in Portuguese, or “Child Health, Food, Nutrition and Development” in English.
ResultsThe KMO coefficient showed acceptable and adequate values to carry out the analysis on the third (0.78), sixth (0.73) and twelfth month postpartum (0.81). According to Bartlett ‘s test of sphericity (χ
2=332.52;
p<0.001), the food groups evaluated were not considered independent and were strongly correlated, parameters needed to carry out the PCA (Supplementary Table 1). The KMOcriterion identified two DPs, named according to their composition: Predominantly healthy DP (PHDP) and predominantly ultra-processed dietary pattern (PUPDP).
Between February-August 2017, there were 394 births. Of the total eligible cases (284), 240 women were recruited to participate in the study. At the end of the 12-month follow-up, losses represented 23.5% of the initial sample, with the main reason, was moving to other cities (Supplementary Figure 2).
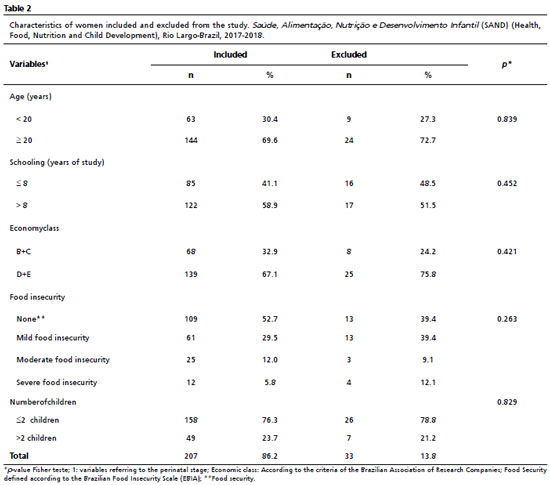
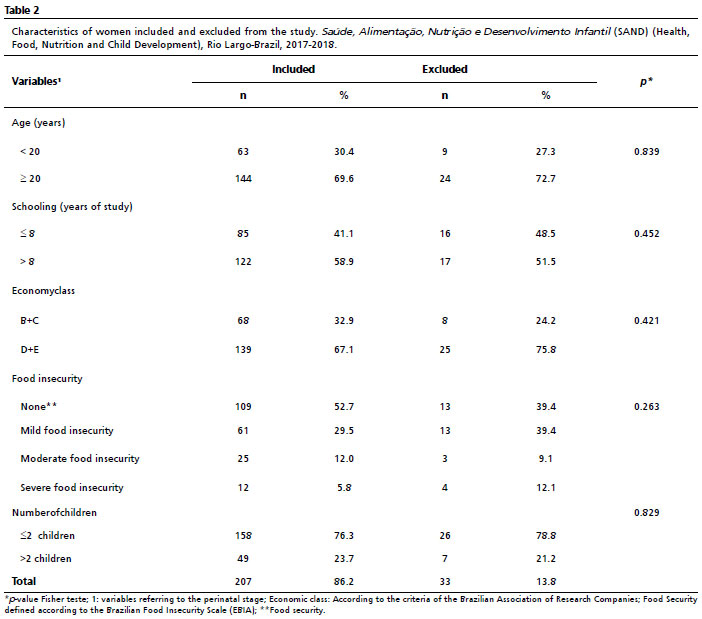
Table 2 describes the characteristics of the population included and excluded from the study; no statistically significant differences were identified between the two groups. The population was composed of around 70% women ≥20 years of age and approximately 60% with >8 years of study. About socio-economic class, most of the women evaluated were on low incomes (67%), according to the criteria adopted. With regard to food insecurity, 29% of the women had mild insecurity, 12% had moderate insecurity and approximately 6% had severe insecurity, according to the score obtained by the EBIA.
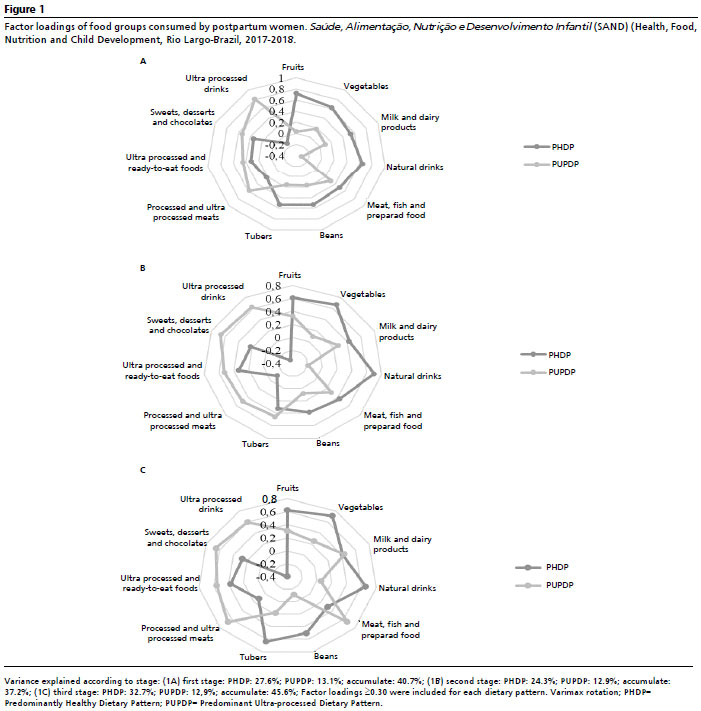
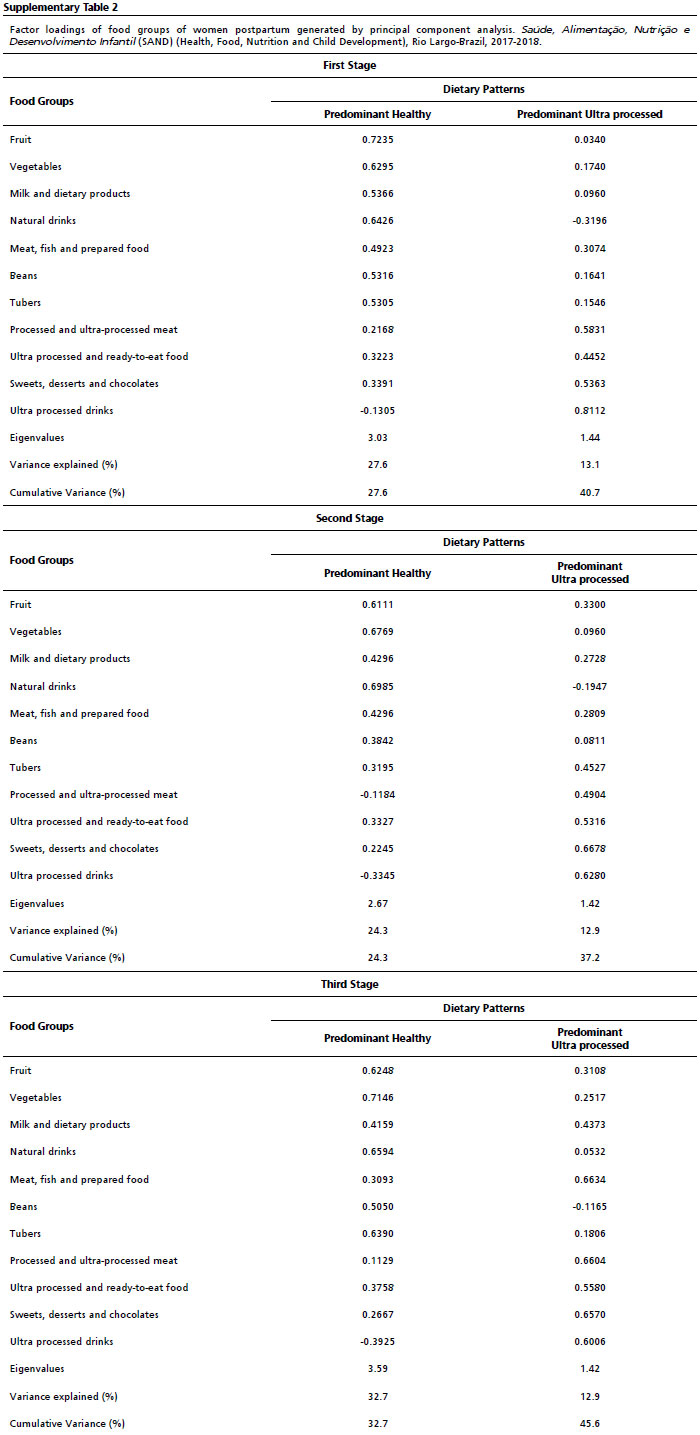
The formation of the two factors and their respective explained variances are presented in Supplementary Table 2 and Figure 1. In the first stage of the study, the PHDP showed higher factor loadings for fruit, vegetables, milk and dairy products, fresh beverages, meat, beans and tubers (Figure 1A). In the second stage, the PHDP showed higher factor loadings for fruit, vegetables, milk and dairy products, fresh drinks, meat and beans (Figure 1B). In the third stage, the PHDP was characterized by higher factor loadings for fruit, vegetables, fresh drinks, beans and tubers (Figure 1C). The PUPDP, in the first stage of the study, showed higher factor loadings for ultra-processed meat, ultra-processed and ready-to-eat food, sweets and cookies and ultra-processed drinks (Figure 1A). In the second stage, the PUPDP showed higher factor loadings for ultra-processed meat, ultra-processed and ready-to-eat food, sweets and cookies, tubers and ultra-processed drinks (Figure 1B). In the third stage, the PUPDP was characterized by higher factor loadings for milk and dairy products, meat, ultra-processed meat, ultra-processed and ready-to-eat food, sweets and cookies and ultra-processed drinks (Figure 1C).
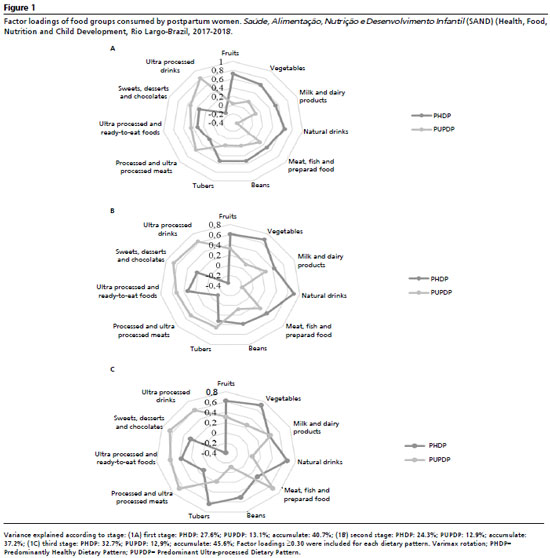
The eigenvalues for the DPs identified, as well as the variances explained according to the periods analyzed, are described in Supplementary Table 2 and Figure 1. It was observed that eigenvalues for PHDP were 3.0, 2.6 and 3.5 in the three stages of the study, respectively; while for PUPDP the eigenvalues were 1.4 for the three stages of the study. It was observed that PHDP explained the greatest variance in the three stages analyzed: 27.6%, 24.3% and 32.7%, respectively, while for PUPDP, the explained variance was 13.1% for the first stage and 12.9% for the second and third stage; the accumulated variance of DP identifies in the three stages analyzed were: 40.7%, 37.2% and 45.6%, respectively (Supplementary Table 2 and Figure 2).
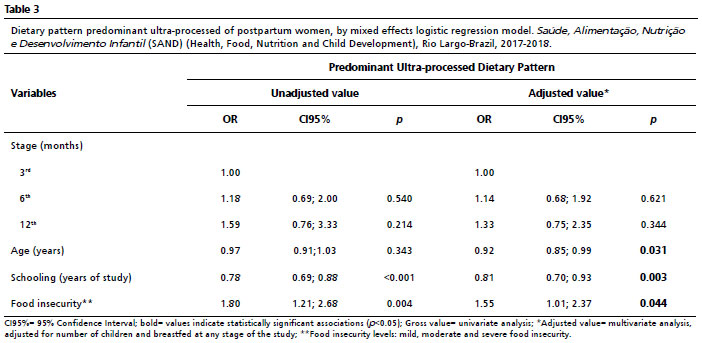
The mixed effects logistic regression evaluated factors related to greater adherence to PUPDP among postpartum women. In relation to the temporal evolution of adherence to PUPDP, no statistically significant changes were observed in adherence at the three time points studied. Regarding greater adherence to PUPDP, an inverse association was observed with age, in years (OR=0.92; CI95%= 0.85; 0.99;
p=0.031), indicating that for each additional year of age, the likelihood of adherence to the DP decreases. Similarly, a higher education level, in years of study, was related to adherence (OR= 0.81; CI95%=0.70; 0.93;
p=0.003), with each one-unit increase in schooling level reducing the likelihood of adherence. Conversely, it is observed that adherence to DP increases with the level of food insecurity (OR= 1.55; CI95%= 1.01; 2.37;
p=0.044). Thus, for each increase of one level in food insecurity (e.g., from food security to mild, from mild to moderate, or from moderate to severe food insecurity), the odds of greater adherence to the PUPDP increase by 55% (Table 3).
DiscussionThis study, developed with data from the first cohort in Alagoas that followed postpartum women, identified two DPs: a composed predominantly of healthy food, PHDP; and a DP composed of predominantly ultra-processed food, PUPDP, with no variation temporal impact on adherence to unhealthy DP throughout follow-up. Regarding the main findings of the study, it is highlighted that the lower the age and level of schooling of the population studied, the greater the adherence to PUPDP and that adherence to PUPDP increases with the level of food insecurity.
The identified DPs were named considering the predominance of the food that formed them, characterized according to their degree of processing. The PHDP was predominantly made up of healthy food. However, it is possible to observe that unhealthy food was also part of this DP, but to a lesser extent. In general, women who are more likely to adhere to a PHDP are more likely to follow the recommendations proposed by the food guide for the Brazilian population, which encourages the consumption of natural and minimally processed food.
2,3The PUPDP was predominantly made up of unhealthy food, such as ultra-processed food. However, healthy food was also included in this DP, but to a lesser extent. Just as it was identified in the PHDP, with regard to unhealthy food. Ultra-processed food are industrial formulations made from the inclusion of ingredients that are harmful to the health when ingested in high quantities, such as sugar, sodium, saturated fat and food additives, which means that individuals who use them as the basis of their diet have an increased risk of developing various types of chronic diseases, such as hypertension, diabetes, cancer, among others.
22,23 A variation in the composition of DP over time was observed with an incorporation of some healthy items in the PUPDP in the second andthird times evaluated, change that indicates the complex and dynamic nature of individuals’ food choices over time.
Studies that evaluated women during pregnancy and/or the postpartum period identified similar DPs.
7,8 Despite different methods of identifying and naming DPs, most analyses show variations, from healthy DPs to DPs characterized by ultra-processed food and drinks. The need for nutritional counseling to avoid increased consumption of ultra-processed food is emphasized, especially during the period analyzed.
7,8 Considering the variances of the PHDP, was the one that best explained the food consumption of this population.
Similar results were found in a population in this stage of life, the healthy DP also best explained the food consumption of the population evaluated.
7 Another study indicated that the DP with the greatest variance and explanatory power of the food consumption of pregnant women evaluated was characterized by saturated and trans fats, sodium, sugars and low in fruit and vegetables.
8 There is scientific evidence in the literature regarding the consequences of eating ultra-processed food on human health,
24 however, studies analyzing the consumption of ultra-processed food during the first year after birth are rarer and more recent.
25The
Pesquisas de Orçamentos Familiares (POF) (Household Budget Surveys) revealed an increase in ultra-processed food in the total calories of the Brazilian population’s diet, contributing approximately 20% of daily calories
11 while there was a decrease in the consumption of freshand minimally processed food in all of the macro-regions in the country.
22This condition is strongly influenced by urbanization, industrialization, and globalization, which facilitate the insertion and availability of ultra-processed food in middle and low-income countries. These factors have favored an increase in the consumption of these products and a decline in the consumption of fresh and minimally processed food.
22A factor that deserves attention in this type of assessment concerns age, which can be identified in our study as being negatively associated with PUPDP. These findings are in line with those of previous studies, in which younger pregnant and puerperal women showed lower adherence to healthy DP when compared to adherence to unhealthy DP.
5,7 It is clear that older women, when evaluating the period between pregnancy and the first year postpartum, have a greater consumption of healthy foods during pregnancy, when compared to younger women.
5In our explanatory model, the effect of level of schooling on adherence to PUPDP was also analyzed. Women with more years of schooling had lower adherence to PUPDP. Awareness of the importance of eating properly increases with greater access to schooling.
5 It is possible to infer a strong and positive association between age and level of schooling, as well as greater adherence to healthier eating behaviors and greater concern for maternal and child health.
10Another point that deserves attention concerns food insecurity, and our findings show that this condition was also related to adherence to the PUPDP. The food insecurity to which the women were subjected, the higher the contribution of ultra-processed products in the composition of the DP adopted, a situation that compromises the adequate supply to meet the maternal and fetal demands of the mother and child.
1 Scientific evidence shows that food insecurity compromises the quantity and quality of the diet perceived as adequate, resulting in changes to the usual DPs of the population. The results of a food consumption study conducted among food insecure women during pregnancy showed a lower consumption of vegetables when compared to food secure women.
13Survival strategies, with a reduction in the quality and quantity of food consumed, have been adopted in situations of food insecurity. In this context, these families begin to replace healthy food, which are often more expensive (fresh food, proteins of high biological value, etc.), with cheaper products of lower nutritional quality (ultra-processed, calorie-dense, with an excess of simple carbohydrates, sodium, and trans fats and low in fiber).
12The consumption of ultra-processed food has grown exponentially in recent years, especially among middle- and low-income countries, increasingly affecting the most socioeconomically vulnerable populations, like the population studied here. The availability of ultra-processed food is high and is increasing, affecting the DPs of the world’s population, which now consists of ultra-processed food.
23 These changes in DPs have led to important changes in the epidemiological profile of the population.
26 The production and high consumption of ultra-processed food also fosters an unsustainable food system, which encourages monocultures, impacts environmental health and degrades food crops.
23,27However, we must emphasize that diet is an important modifiable risk factor and altering a pathogenic DP by adopting a healthy diet has a positive impact on human health, preventing illness and early death.
27Considering the nutritional recommendations at this stage of the life cycle, consumption should be assessed in a targeted way. Certainly, food and nutritional guidance for women during prenatal care, the puerperium, the immediate postpartum period and throughout the first year is considered strategic. However, food choices are not only determined by the recognition of nutritional and physiological needs, but above all, by physical and financial access to food. Therefore, it is essential to improve the access of food insecurity of families to healthy food.
28Emancipatory food and nutrition education is therefore necessary, together with the implementation of public policies that have an impact on improving the population’s access to healthy diets before, during and after pregnancy.
29 Taxes on ultra-processed food have been implemented in several countries, achieving positive results in terms of reducing the population’s consumption of these products. Tax subsidies aimed at stimulating the production and marketing of fresh/minimally processed food have the potential to improve access to healthy food and positively shape the composition of DPs.
30This study has some limitations, such as the sample size, which may have had an impact on the effects identified, suggesting caution when discarding the statistically non-significant associations found. Also, it is noteworthy the non-probabilistic sampling approach, which may cause bias to the selection, including only those who have more access to health services and possibly greater health care. However, it is important to emphasize that all women who gave birth in the only public hospital in the city were included.
It is worth noting that we did not include a group of food derived from rice, bread, and corn in our analysis due to their very low factor load. While this decision was based on strict statistical criteria, the absence of these items could potentially affect the results of diets that frequently include them. Additionally, by analyzing the DP as a dichotomous variable and assigning a single pattern to all, we may have disregarded the individual’s participation in the other DPs. Finally, the study was carried out with low-income women, and the results may need to be validated for other social classes, ethnicities, or specific people.
Strengths include the fact that this is a prospective study carried out with rigorous data quality control. Considering its internal validity, the results can be extended to other locations since the characteristics of the city studied are similar to those of many other Brazilian cities with a similar HDI, especially in the Northeast region. The food consumption assessment tool used was validated for the Brazilian population, with more than 100 items that include preparations and regional food that are part of the eating habits of the population studied. The mixed-effects logistic regression model developed made it possible to assess intra-individual variations and the effect of time on adherence to the DP, which favors the analysis of longitudinal data. The analysis technique used takes into account temporal variation, as well as the correlation between successive measurements.
This cohort study provided a better understanding of DP among low-income women over a year after childbirth, as well as factors that influence adherence, which did not vary over the period evaluated.
The adherence to PUPDP increases with the level of food insecurity. The analytical approach adopted also showed that the higher age and level of schooling decreases the adherence to this DP. These findings provide additional support for the association between the levels of food insecurity with adherence to PUPDP, suggesting the need for effective measures to ensure food security and the human right to adequate food. In relation to the women’s health care and care network, efficient and decisive responses are recommended that promote food and nutritional information and favor access to healthy food, especially among the most biologically and socially vulnerable population groups.
References1. Marshall NE, Abrams B, Barbour LA, Catalano P, Christian P, Friedman JE,
et al. The importance of nutrition in pregnancy and lactation: lifelong consequences. Am J Obstet Gynecol. 2022; 226 (5): 607-32.
2. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Guia alimentar para a população brasileira. 2
nd ed., 1.reimpr. Brasília (DF): Ministério da Saúde; 2014. [access in 2023 Nov 16]. Available from:
https://bvsms.saude.gov.br/bvs/publicacoes/guia_alimentar_populacao_brasileira_2ed.pdf3. Ministério da Saúde (BR). Fascículo 3 Protocolos de uso do Guia Alimentar para a população brasileira na orientação alimentar de gestantes. Brasília (DF): Ministério da Saúde; 2021. [access in 2023 Nov 16]. Available from:
https://nutriacao.saude.ms.gov.br/files/nutriacao/arquivos/3d6a048bf01758a5.pdf4. Swinburn BA, Kraak VI, Allender S, Atkins VJ, Baker PI, Bogard JR,
et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. The Lancet. 2019; 393 (10173): 791–846.
5. Poulain T, Spielau U, Vogel M, Dathan-Stumpf A, Körner A, Kiess W,
et al. Changes in diet from pregnancy to one year after birth: a longitudinal study. BMC Pregnancy Childbirth. 2021; 21 (1): 600
6. Lebrun A, Plante AS, Savard C, Dugas C, Fontaine-Bisson B, Lemieux S,
et al. Tracking of Dietary Intake and Diet Quality from Late Pregnancy to the Postpartum Period. Nutrients. 2019; 11: 2080.
7. Castro MB, Freitas Vilela AA, Oliveira AS, Cabral M, Souza RAG, Kac G,
et al. Sociodemographic characteristics determine dietary pattern adherence during pregnancy. Public Health Nutr. 2016; 19 (7): 1245-51.
8. Mota Santana J, Oliveira Queiroz VA, Pereira M, Paixão ES, Brito SM, Barbosa dos Santos D,
et al. Associations between Maternal Dietary Patterns and Infant Birth Weight in the NISAMI Cohort: A Structural Equation Modeling Analysis. Nutrients. 2021; 13 (11): 4054.
9. Bedrick BS, Eskew AM, Chavarro JE, Jungheim ES. Dietary Patterns, Physical Activity, and Socioeconomic Associations in a Midwestern Cohort of Healthy Reproductive-Age Women. Matern Child Health J. 2020, 24 (10): 1299–1307.
10. Jardí C, Aparicio E, Bedmar C, Aranda N, Abajo S, March G,
et al. Food Consumption during Pregnancy and Post-Partum. ECLIPSES Study. Nutrients. 2019; 11 (10): 2447.
11. Louzada ML, Cruz GL, Silva KAAN, Grassi AGF, Andrade GC, Rauber F,
et al. Consumo de alimentos ultraprocessados no Brasil: distribuição e evolução temporal 2008-2018. Rev Saúde Pública. 2023; 57.
12. Morales ME, Berkowitz SA. The Relationship between Food Insecurity, Dietary Patterns, and Obesity. Curr Nutr Rep. 2016; 5 (1): 54-60.
13. Gonzalez-Nahm S, Østbye T, Hoyo C, Kravitz RM, Benjamin-Neelon SE. Association between food security, diet quality, and dietary intake during pregnancy in a predominantly African American group of women from North Carolina. J Acad Nutr Diet. 2021; 122 (3): 565-72.
14. Programa das Nações Unidas para o Desenvolvimento (PNUD). Instituto de Pesquisa Econômica Aplicada (IPEA). Fundação João Pinheiro (FJP). Perfil - Rio Largo, AL | Atlas do Desenvolvimento Humano no Brasil 2010. Brasília (DF): PNUD, IPEA, FJP; 2013. [access in 2023 Nov 16]. Available from:
https://www.undp.org/pt/brazil/desenvolvimento-humano/atlas-do-desenvolvimento-humano-no-brasil15. Molina MCB, Faria CP, Cardoso LO, Dremer M, Velasquez-Meléndez JG, Gomes ALC,
et al. Diet assessment in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Development of a food frequency questionnaire. Rev Nutr. 2013; 26 (2): 167-76.
16. Soleimani D, Ranjbar G, Rezvani R, Goshayeshi L, Razmpour F, Nematy M. Dietary patterns in relation to hepatic fibrosis among patients with nonalcoholic fatty liver disease. Diabetes Metab Syndr Obes. 2019; 12: 315-24.
17. Rinaldi AEM, Conde WL. Secular trends in dietary patterns of young children in Brazil from 1996 to 2006. Public Health Nutr. 2017; 20 (16): 2937-45.
18. Segall-Correa AM, Marin-Leon L, Melgar-Quiñonez H, Perez-Escamilla R. Refinement of the Brazilian Household Food Insecurity Measurement Scale: Recommendation for a 14-item EBIA. Rev Nutr. 2014; 27 (2): 241-51.
19. Word Health Organization (WHO). Young People´s Health - a Challenge for Society. Report of a WHO Study Group on Young People and Health for All. Geneva: WHO; 1986. (Technical Report Series 731). [access in 2023 Nov 16]. Available from:
https://iris.who.int/handle/10665/4172020. Associação Brasileira de Empresas de Pesquisa (ABEP). Critério de Classificação Econômica Brasil 2015: atualização da distribuição de classes para 2016. [access in 2023 Nov 16]. Available from:
https://www.abep.org/criterio-brasil21. Fausto, MA, Carneiro M, Antunes CMDF,Pinto JA, Colosimo EA. Mixed linear regression model for longitudinal data: application to an unbalanced anthropometric data set. Cad Saúde Pública.2008; 24: 513-24.
22. Silva MAL, Louzada MLC, Levy RB. Disponibilidade domiciliar de alimentos regionais no Brasil: distribuição e evolução 2002-2018. Segur Alim Nutr. 2022; 29 (00): 022007.
23. Monteiro CA, Cannon G, Lawrence M, Costa Louzada ML, Pereira Machado P. Ultra-processed foods, diet quality, and healthusingthe NOVA classification system. Rome: Food and Agriculture Organization (FAO); 2019. [access in 2023 Nov 16]. Available from:
https://openknowledge.fao.org/server/api/core/bitstreams/5277b379-0acb-4d97-a6a3-602774104629/content24. Oliveira JS, Menezes RCE, Almendra R, Lira PIC, Aquino NB, Souza NP,
et al. Unhealthy food environments that promote overweight and food insecurity in a Brazilian metropolitan area: A case of a syndemic? Food Policy. 2022; 112: 102375.
25. Oliveira PG, Sousa JM, Assunção DGF,
et al. Impacts of Consumption of Ultra-Processed Foods on the Maternal-Child Health: A Systematic Review. Front Nutr. 2022; 9: 821657.
26. Gorski MT, Roberto CA. Public health policies to encourage healthy eating habits: recent perspectives. J Healthcare Leadersh. 2015; 7: 81-90.
27. Willett W, Rockström J, Loken B, Springmann M, Lang T,Vermeulen S,
et al. Food in the Anthropocene: the EAT–Lancet Commission on healthy diets from food systems. Lancet. 2019; 393 (10170): 447-92.
28. Claro RM, Maia EG, Costa BVL, Diniz DP. Food prices in Brazil: prefer cooking to ultra-processed foods. Cad SaúdePública. 2016; 32 (8): e0014715.
29. Boelsen-Robinson T, Blake MR, Backholer K, Hettiarachchi J, Palermo C, PeetersA,
et al. Implementing healthy food policies in health services: A qualitative study. Nutr Diet. 2019; 76 (3): 336-43.
30. Peñalvo JL, Cudhea F, Micha R,Rehm CD, Afshin A, Whitsel L,
et al. The potential impact of food taxes and subsidies on cardiovascular disease and diabetes burden and disparities in the United States. BMC Med. 2017; 15 (1): 208
Authors’ contributionSoares LL: designed the study, analyzed the data and discussed the synthesis of the analyses, wrote the first draft of the manuscript.
Longo-Silva G: coordinated the project, supervision of the first draft of the manuscript.
Silveira JAC: coordinated the project, analyzed the data and discussed the synthesis of the analyses, supervision of the first draft of the manuscript.
Silva-Neto LGR: supervision of the first draft of the manuscript.
Freire JKS, Menezes RCE: analyzed the data and discussed the synthesis of the analyses.
Marinho PM: analyzed the data and supervision of the first draft of the manuscript.
Leal VS, Oliveira JS: supervision of the first draft of the manuscript.
Clemente APG: provided substantive reviews of the second and subsequent drafts of the manuscript.
All authors approved the final version of the article and declare no conflict of the interest.
Received on March 18, 2024
Final version presented on Augusto 26, 2024
Approved on August 29, 2024
Associated Editor: Paola Mosquera


 ; Giovana Longo-Silva 2
; Giovana Longo-Silva 2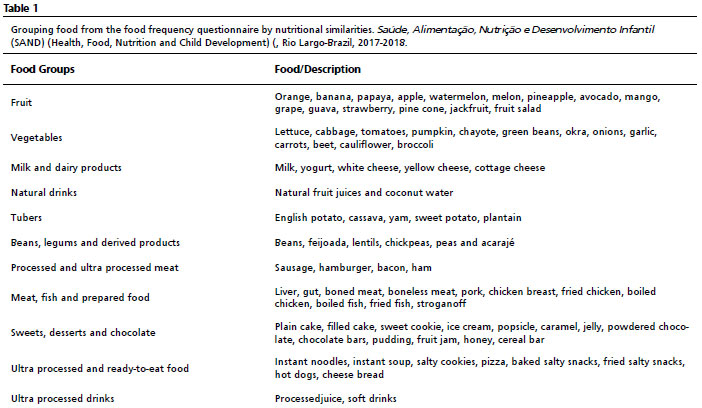






 Ler em português
Ler em português