ABSTRACT
OBJECTIVES: to analyze the clinical guidelines of countries that offer abortion in Primary Health Care (PHC), aiming to understand how the service delivery and the performance of PHC professionals occurs in different scenarios, to reflect on the viability of this offer in Brazil.
METHODS: narrative review carried out from the Global Abortion Policies Database platform, which gathers comprehensive information on abortion laws, regulations and clinical guidelines. Clinical guidelines from countries where abortion is performed at the first level of care were selected, in English, Spanish and Portuguese.
RESULTS: 26 countries were identified and 13 were included in the study. In general, abortion is performed in PHC in the first trimester, using medication or aspiration techniques, by different professional categories depending on the location, without the need for prior ultrasound.
CONCLUSIONS: the study of international experiences shows that it is possible to provide abortion in PHC services using the existing workforce and structure, in accordance with the recommendations of the World Health Organization to facilitate access to the procedure. In Brazil, despite the problems related to access to legal abortion, its performance remains restricted to hospitals. It is expected to contribute to the reformulation of regulations regarding abortion in the country.
Keywords:
Induced abortion, Legal abortion, Health services accessibility, Primary health care, delivery of health care, Practice guideline
RESUMO
OBJETIVOS: analisar as diretrizes clínicas de países que ofertam a realização de aborto na Atenção Primária à Saúde (APS), buscando compreender como se dá a organização dos serviços e atuação dos profissionais da APS em diferentes cenários, de modo a ampliar a reflexão sobre a viabilidade desta oferta no Brasil.
MÉTODOS: revisão narrativa realizada a partir da plataforma Global Abortion Policies Database, que reúne informações abrangentes sobre leis, regulamentações e diretrizes clínicas referentes ao aborto. Foram selecionadas as diretrizes clínicas de países em que o aborto é realizado no primeiro nível de atenção, nos idiomas inglês, espanhol e português.
RESULTADOS: 26 países foram identificados e 13 foram incluídos no estudo. De modo geral, o aborto é realizado na APS no primeiro trimestre, com uso de medicamentos ou técnicas de aspiração, por categorias profissionais variadas conforme a localidade, sem necessidade de ultrassonografia prévia.
CONCLUSÕES: a análise das experiências internacionais mostra que é possível prover aborto em serviços de APS utilizando a força de trabalho e estrutura existentes, conforme as recomendações da Organização Mundial da Saúde para facilitação do acesso ao procedimento. No Brasil, apesar dos problemas relacionados ao acesso ao aborto legal, sua realização segue restrita a hospitais. Espera-se contribuir para a reformulação das regulamentações acerca do aborto no país.
Palavras-chave:
Aborto induzido, Aborto legal, Acesso aos serviços de saúde, Atenção primária à saúde, Prestação de cuidados de saúde, Guia de prática clínica
IntroductionIn 2022, the World Health Organization (WHO) updated its clinical guidelines concerning abortion care, and highlighted the quality of care as a structural aspect for its recommendations. Accessibility is recognized as one of the main components of quality, and presupposes that healthcare could be obtained timely, at a viable cost, in a geographically accessible location, where resources and techniques that are necessary for their execution are available. Accessibility is understood as aspects of the structure of a given healthcare service or system that are mandatory to achieve healthcare itself, whilst access is the way that people experience these characteristics.
2Although it is a simple procedure, with low potential of complications, considered an essential service for reproductive health, several barriers can be observed in the access to abortion across the world, including situations in which it is provided for by law. Some examples are the absence of precise information on availability of abortion, biased counseling, imposition of mandatory waiting periods for the confirmation of a decision of women, the requisition of third party authorization, unavailability of essential medications and restrictions related to facilities and health professionals that may provide the abortion.
1Since 2003, when the first edition of the technic document entitled “Safe abortion: technical & policy guidance for health systems”
3 was published, the WHO indicates the offer of abortion in Primary Healthcare (PHC) services as an important mechanism of facilitation of access to the procedure, highlighting that developing these services and qualifying their professionals are some of the most relevant investments that can be made. In the 2022 guidelines, the provision of abortions in PHC is still mentioned as a necessary, safe and effective strategy to promote equitable access. Both medication abortion and vacuum aspiration, considered methods of choice for the execution of the procedure in pregnancies of up to 14 weeks, can be performed with safety in this level of attention.
1Brazil’s Law is, worldwide, one of the most restrictive in relation to abortion, the latter being allowed only in pregnancies that occurred after a rape, when the pregnant women is at risk of life or in cases of anencephaly.
4,5 Even in this cases, the offer of the procedure in the Unified Health System (SUS – Portuguese acronym) is limited and distributed unequally in the national territory, being present in less than 4% of municipalities and concentrated on those more populous and with a higher human development index. Only 26.7% of female population of childbearing age in the country reside in municipalities that offer legal abortion, and those women present a rate of execution of the procedure almost five times higher than those of women residing in municipalities without the offer of the procedure.
6,7The regulation of reference services for interruption of pregnancy cases provided by law can be understood as one of the reasons for the inequality of access observed, since it preconizes that its organization is restricted to hospitals, maternities and other urgency and emergency services with uninterrupted operation, 24 hours a day and seven days per week, among other requisites.
8 In case of being adopted in Brazil, the WHO abortion care guidelines in PHC services, considering the current capacity implemented, legal abortion could be offered in at least 67% of Brazilian municipalities, were 94.3% of women of childbearing age resides.
The absence of access to legal abortion, besides constituting a violation of human rights, may generate severe consequences that are potentially fatal, such as the use of unreliable methods for interrupting a pregnancy. Observing the potential of radical change in the Brazilian panorama concerning accessibility to abortion care, this article aims to analyze clinical guidelines of countries that offer this procedure in the first level of care, in attempt of understanding the organization of services and acting of PHC professional in different scenarios, so that the discussion on the availability of this service in Brazil can be expanded.
MethodsNarrative review of clinical guidelines of countries that offer abortion care in PHC services, which started with the platform Global Abortion Policies Database (GADP),
9 launched in 2017 by WHO and collaborators. GADP is a database of free access that gathers detailed information on laws, regulations and clinical protocols related to abortion in WHO and United Nations (UN) country members. All information present in this database were extracted of source-documents that can be accessed from the platform.
9The database possesses functionalities that allow filtrating countries according to some characteristics. For the identification of countries that offer abortion care in PHC services, we used a specific filter for this information (“
Clinical and service-delivery aspects of abortion care - Where can abortion services be provided - Primary health-care centers”). The clinical guidelines of abortion care (and specific regulations about abortion, when essential information were missing on the guidelines) in the identified countries were accessed, from the platform, with further search for updated versions in the governmental official websites. Those available in Spanish, Portuguese or English were included in the present study. The identification and selection of countries were performed in April 2023.
The analysis of clinical guidelines of countries included in the study, carried out from April to June 2023, aimed to extract data that allow comprehending the functioning of abortion in PHC services, as well as the general characterization of the regulation of access to abortion in those countries. Some of the WHO current recommendations,, directly or indirectly related to the access to the procedure, were used as lens analysis. The document “Abortion care guideline”,
1 published by WHO in 2022, presents a group of recommendations, based on scientific evidence that attempted to induce qualified care to abortion situations in different scenarios. The recommendations, are clustered in four domains, namely: laws and policies, provision of services, clinical management and self-management.
With regard to laws, we investigated the situations in which abortion is allowed by law, the limits of gestational age for its execution, the existence of a mandatory waiting period between the request and execution of the procedure, and the mandatory authorization of guardians for minors. In relation to provision of services, we observed the procedures offered in the first level of care (medical and/or surgical abortion), the professionals qualified for its execution and the limit of gestational age that allows the abortion to be done at PHC. With regard to clinical practices, we verified the availability of medicines considered essential, the obligation of ultrasound exam before the procedure and the possibility of self-management at home.
1Data collected were compared to Brazilian regulations
4,5,8,10 whenever possible. Considering the strict usage of documents of public access, this study was not submitted to the appraisal of research ethics committees.
ResultsOf the 193 countries recognized by UN, 26 offers abortion in PHC services, whilst 11 professedly do not offer this procedure in the first level of care; for 156 countries, there is no specific information available.
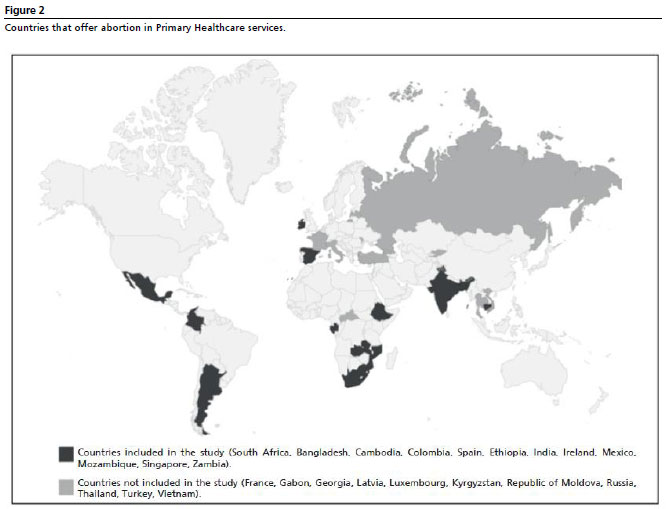
9 Of the 26 countries that perform abortions in PHC services, 13 have clinical guidelines in Portuguese, English or Spanish, being included in this study. Figure 1 demonstrates the process of selection of guidelines, and Figure 2 shows the countries that offer abortion in PHC.
The documents included in this review are mostly clinical guidelines published by government departments, which aim to orientate the performance of health professionals in the provision of legal abortion.
11-23 For Mozambique and Colombia, it was necessary to add laws that modified the situations in which abortion is allowed after the date of publication of guidelines;
24,25 for Spain, due to the inexistence of a national guideline, we used the organic law of sexual and reproductive health and voluntary interruption of pregnancy,
26 the decree of guarantee of quality of assistance of voluntary interruption of pregnancy
27 (both with national broadness), and the clinical protocol of one of the autonomous communities of the country
22 (Canary Islands, since it is the only available in GAPD platform in Spanish).
The results are disposed into three topics: Characterization of laws and policies related to abortion in countries that offer its execution in PHC services; Aspects related to the provision of abortion care services in countries that offer its execution in PHC; and Aspects related to clinical management and self-management of abortion in countries that offer its execution in PHC.
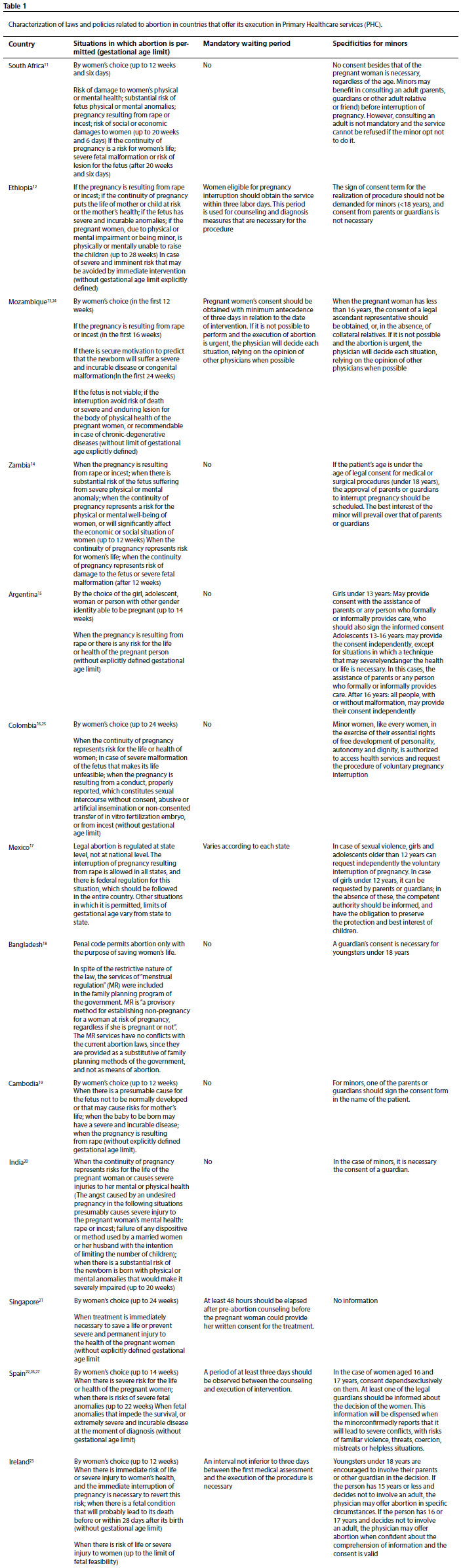
Characterization of laws and policies related to abortion in countries that offer its execution in PHC servicesEight countries allow abortion by women’s choice, being the limit of gestational age mostly placed in the transition of the first to the second trimester of pregnancy.
11,15,19,23,24,26 Colombia and Singapore stand out for authorizing abortion by women’s choice up to 24 weeks of pregnancy.
21,25 In Mexico, although the regulation of the procedure occurs in sub-national level, the Supreme Court of Justice decriminalized abortion in up to 12 weeks in national level, averting women or professionals to be punished for its execution in the entire country.
17 India, Zambia and Ethiopia allow the execution of abortion in specific situations and the legal permissives of the first two are broader, since they include cases in which pregnancy stand out as damages to mental health.
12,14,20 Bangladesh situation is worth to be presented separately, since abortion is allowed in the country only to save women’s life, but menstrual regulation (MR) is comprehended as a strategy of reproductive planning, and not as means of abortion.
18Whilst the mandatory waiting period is current in four countries,
13,21,23,26 in Colombia and Argentina a maximum term is legally established, in which the procedure should be performed (respectively, from five to ten days after the first consultation), aiming to protect the requesting person from medical, bureaucratic and legal barriers that may delay the access.
15,16 The Ethiopian guidelines are not clear whether the interval of three days, in which counseling and diagnosis measures occur, is a mandatory waiting period.
12Regarding abortion in minors, in three countries the involvement of parents or guardians is not necessary for the authorization of the procedure,
11,12,16 and in four countries this authorization is necessary.
14,18-20 Spain, Ireland, Argentina, Mexico and Mozambique present varied targeting per age group, defining an age from which the consent could be provided independently (12 years in Mexico and 16 in the others).
15,17,23,24,26Table 1 presents the details of laws and policies related to abortion in 13 countries included in the study.
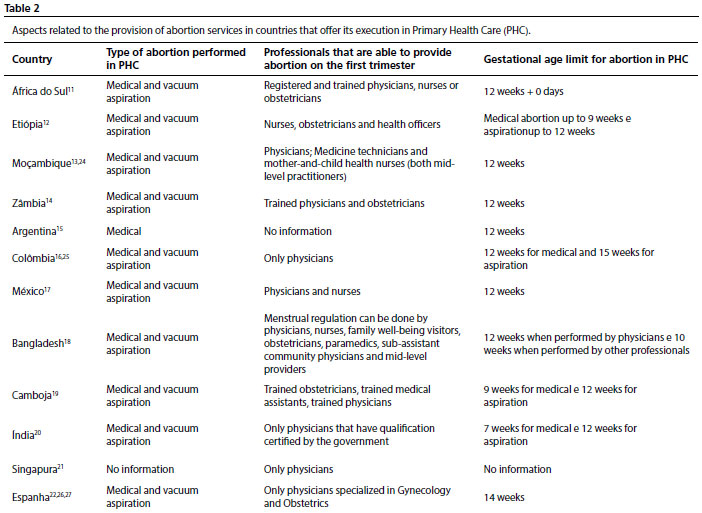
Aspects related to the provision of abortion care services in countries that offer its execution in PHCThe guidelines researched mostly indicate the possibility of execution of medical abortion and vacuum aspiration in PHC,
11-14,16-20,22 with a limit of 12 weeks for the provision of abortion in this level of care.
11-15,17-20 Some countries establish a lower limit of gestational age for medical abortion than vacuum aspiration abortion.
12,19,20 Such limits find justification in previous WHO publications and scientific evidence available in the period of publication of these guidelines, which established safety and effectiveness of medical abortion only up to nine weeks.
1With regard to the professionals that can provide abortion in the first trimester, some countries restrict the practice only to physicians,
16,20,21,23,27 whilst others include nurses,
17 obstetricians
11,14 and mid-level practitioners.
11,12,13,18,19 The guidelines of Argentina do not approach this information clearly (using the term “health professionals”).
15 Only Spain restricts the practice of abortion of first trimester to physicians specialized in Gynecology and Obstetrics.
27 Table 2 resumes the individualized information of surveyed countries.
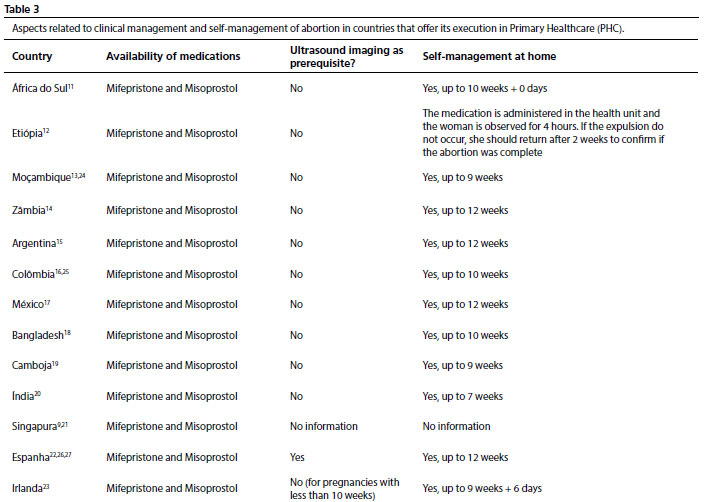
Aspects related to clinical management and self-management of abortion in countries that offer its execution in PHCBoth mifepristone and misoprostol are registered in all countries included in the study. With regard to the execution of ultrasound exam, only Spanish regulations determine this exam as a mandatory prerequisite for the execution of abortion.
27 Most researched guidelines contemplate the possibility of self-management of abortion at home, with variations in the maximum gestational age allowed (between seven and 12 weeks).
11,13-15,17-20,22,23 The information related to this topic are consolidated in Table 3.
DiscussionWhen documents are used as data source, it is important to comprehend them as means of communication, and not only as an information repository; thus, aspects as authorship and context in which they were produced should be valued.
28 Of the 13 countries included in the study, four are classified by UN as having very high human development index (HDI) (in descending order of HDI: Ireland, Singapore, Spain and Argentina), three present high HDI (Mexico, Colombia and South Africa), other four present medium HDI (Bangladesh, India, Cambodia and Zambia) and two present low HDI (Ethiopia and Mozambique).
29 By means of comparison, Brazil is classified as a country with high HDI, scoring the 87º position in the 2021/2022 report, between Mexico (86º) and Colombia (88º).
29The clinical guidelines of several countries were published in partnership with or counted on the support of organizations that act in the defense of reproductive rights, such as the United Nations Population Fund (UNFPA) and Ipas (an international, non-governmental organization that seeks to increase access to safe abortions and contraception), or WHO itself. This support is mentioned in all documents, except for Ireland, Spain and Singapore.
11-20Notably, these three countries are the only that present very low maternal mortality ratio (MMR).
30 All others present low or moderate MMR,
30 and describe in their guidelines a still unfavorable scenario for maternal mortality, with deaths by abortion standing among the main causes. To this extent, they explicitly signalize the need for ensuring the access to safe abortions whenever provided for by law, as a manner of averting maternal deaths.
11-20With regard to laws and policies, the WHO recommends abortion to be excluded from penal codes, since the criminalization does not decrease its occurrence, but increase health risks associated with clandestine and unsafe procedures, affecting women of higher vulnerability situation in a disproportionate manner.
1 In the same way, the organization has recommendations that are opposite to laws and regulation that restrict abortions to determinate situations or establish gestational age limits, as well as practices that impair the access to the procedure, such as mandatory waiting periods and the need for third party authorization.
1When analyzing the characterization of laws and policies related to abortion in countries included in the study, it is possible to identify some guidelines with a discourse more focused on the defense of reproductive autonomy, such as in the publications of Argentina, Colombia and Mexico – which are the most recent due to legal changes that occurred in the last four years.
15,17,25 These countries exemplify the movement of change that has been observed in Latin America, previously characterized by very restrictive laws and highly patriarchal societies.
31 Bangladesh and India are in a distinct situation: relaxation of laws observed in the access to abortion seem to be primordially directed for the prevention of maternal deaths, not prevailing in the guidelines a valorization of reproductive autonomy.
18,20 At the same time, the Human Development Report 2021/2022 evidences that these two countries are classified as having a diminished equality between men and women, in relation to HDI results.
29When comparing the Brazilian regulation with the countries included in this study, we observe a more restrictive law, with only three legal permissives for abortion.
4,5 There is no prevision of mandatory waiting period, although the authorization of parents or guardians is required in order to request the procedure for minors.
8This is a particularly sensitive topic in the country, considering the elevated incidence of pregnancies in adolescence, with a high rate of pregnancies resultant from rape in this age group.
32With regard to the provision of abortion care services, the WHO recommends vacuum aspiration in pregnancies of up to 14 weeks to be performed by general practitioners or specialized physicians, nurses and obstetricians, as well as other professional categories not regulated in Brazil, such as professionals of traditional and complementary medicine and associated practitioners.
1 Medical abortion in pregnancies of up to 12 weeks, on the other hand, may be performed by all of these professional categories, also by community health agents, pharmacy workers, pharmaceutical professionals and nursery technicians.
The strategy of redistribution of tasks between members of a health professional team is called “task shifting”, which allows less specialized professionals to perform functions that are traditionally carried out by other professionals with higher graduation. This strategy is encouraged by WHO as a way of ensuring the right to health. It is perceived that restrictions concerning professional categories that can provide abortions are higher in countries with very high or high HDI, which probably reflects a higher availability of higher education professionals. The WHO affirms that such restrictions are inconsistent in relation to its recommendations, since they are arbitrary and not based on evidence, promoting risk of limitation of access to the procedure.
1In Brazil, the law describes abortion as a medical act.
4 The regulation of reference services for pregnancy interruption in cases provided for by law, on the other hand, establishes that “the multidisciplinary health team should be composed of, at least, obstetricians, anesthetists, nurses, social workers and/or psychologists”.
8 That is, besides there is no express restriction of the performance of the procedure to physicians specialized in Gynecology and Obstetrics, it is necessary that this kind of professional integrates the teams of reference services.
Concerning aspects related to clinical management and self-management of abortion assessed in this study, the WHO defines mifepristone and misoprostol as essential medicines for health systems,
33 and do not recommend ultrasound exams as pre-requisites for the execution of abortions, considering that it may limit the access to the procedure in contexts that this exam is hard to be performed. It is also recommended that the self-management of medical abortion in up to 12 weeks, that is, the execution by women themselves, should be recognized as a legitimate strategy and the clinical protocols should be adapted in order to ensure this possibility.
1Such recommendations are observed in the great majority of assessed guidelines, with rare exceptions within the results. The situation of Brazil differs from the studied countries in several aspects: the abortion, both medical and surgical, is considered a medical procedure; mifepristone is not regulated in the Brazilian Health Regulatory Agency; and misoprostol is a medicine under special control.
34 The execution of ultrasound exams is prescribed in the procedure of justification and authorization of pregnancy interruption in cases provided for by law,
8 and in 2020 ordinances were established (already rescinded) updating this procedure, one of which established that “the health team should inform the possibility of visualizing the embryo or fetus by means of ultrasound imaging”.
25According to what was mentioned in the beginning of the discussion, the documents should be understood as means of communication, and their authorship and context matter
28: in this case, talking about the possibility of visualization of the fetus or embryo seems to be contradictory in relation to the assurance for women to the right of not seeing it – which is explicitly recommended in Argentinian and Irish guidelines.
15,23 At the time of release of this ordinance, Brazil had a government with authoritarian profile ruling the country, recognized by anti-gender policies.
36PHC and abortion: beyond the accessThe access of first contact is one of the four essential attributes of PHC, denoting that this level of care should be the preferential gateway of individuals in the health system each time medical care is necessary, and this gateway should be of easy access. The inexistence of an easily accessible gateway may lead to delays or unavailability of adequate care, with consequent increase of costs and risks to health.
2 Abortion is a procedure sensitive to time – that is, the later it is performed, the higher are the associated risks – , one of the reasons that makes access such a relevant question.
1One of the characteristics that facilitate the access to PHC services is their geographical location next to communities. In Brazil, according to what Jacobs demonstrated, the concentration of services that perform legal interruption of pregnancy is a barrier of access,
37 however the country has conditions to solve this issue by means of the offer of the procedure in PHC services: whilst in 2021 the legal interruption of pregnancies resulting from rapes (main cause of legal aborting) was only performed in 55 municipalities, in case of the service was provided in PHC units, considering WHO recommendations, this number would be expanded to 3741 municipalities in Brazil.
7The benefits related to the provision of abortions in PHC services, however, are not limited to access; other essential PHC attributes also can be understood as potentialities.
38 Longitudinality presupposes that PHC services are recognizes by the population as a continued source of care over time, leading to the building of a bond and mutual confidence between patients and health professionals.
2 This sense of confidence can lead women to feel more comfortable to share the experience of sensitive situations such as a pregnancy resulting from sexual violence. Continued care is also strategic for the execution of essential actions for abortion care, such as the prophylaxis of sexually transmitted diseases and the institution of post-abortion contraception.
Comprehensiveness concerns the group of services offered in PHC, which should be broad, making possible the approach of the most frequent and relevant healthcare needs of the population. The actions offered by PHC should provide an integrative care, both in perspective of the biopsychosocial aspect of health-disease processes and the continuum of actions of health promotion, prevention, treatment and rehabilitation.
2 Abortion situations are often complex, benefiting from a integrative view on the person who demands it. Moreover, the proposition of the offer of abortion in PHC services is not limited to the mere execution of the procedure as it may signal a qualification of reproductive health care as a whole, when adding to community services the debate about health promotion and prevention in this area.
Finally, the coordination of care, the fourth essential PHC attribute, denotes the responsibility of this level of care over its users, independently of the site of the healthcare network in which they are located.
2 Naturally, not every abortion could be performed in PHC services, considering the preconized gestational age limits and situations that involve risk of life for women, in which hospital care will be necessary. Therefore, PHC would have an essential role in the coordination of the itinerary of people in healthcare networks according to their needs, ensuring the access to the procedure by means of formal reference mechanisms.
The provision of abortion in PHC services is still a poorly studied subject in Brazil, with scarce publications, making the survey in experiences from other countries relevant, which may be a model for the implementation of this practice in the country. It is worth highlighting, thus, some guidelines that may be of special interest, such as those from Latin American countries
15-17 (due to recent publications and similarities with Brazil), the guideline from India
20 (which brings a systematized proposal of qualification for new providers), from Ireland
23 (which starts with a list of recommendations based on evidence, and values the acting of multidisciplinary team in the counseling and follow-up of women, although abortion itself is only performed by physicians).
Ireland is the country with the highest number of documents of the experience of provision of abortion in PHC services in the scientific literature. After the modification of law in 2018, a model of integrative care to the existing healthcare infrastructure was developed, and abortion started to be executed in maternities and community services.
39 A multidisciplinary task force was responsible by the awareness and qualification of PHC physicians and the elaboration of technical protocols.
39 The interruption of pregnancies with less than ten weeks is performed predominantly in PHC, unless there are clinical conditions that require hospitalization, and the initial results evidenced the success of the procedure in 98,1% of cases.
40 The professionals highlight that the collaborative approach between government and medical community, as well as the financial incentive, were essential for the success of the experience.
41The nature of this study, carried out from the analysis of clinical guidelines, does not comprise the investigation of results originated from the practice of all included countries, the reason by which we indicate the need for a systematic review of literature about the execution of abortion in PHC services. As other limitations that may be highlighted, we mention the non-inclusion of a significant group of countries in which abortions in PHC are performed, due to the language of publication of guidelines; possible flaws of GADP platform in the detection of countries that offer the procedure in this level of attention; the several formats of PHC observed (which may impair the replication of the assistance model), and the inclusion of some guidelines published five years ago or more, for which there is no apparent regular updates.
In spite of the mentioned limitations, the analysis of international experiences makes it clear that it is possible to provide abortion in PHC services, both medical and vacuum aspiration, using the preexisting workforce and structure. There is a relative consensus on the fact that the abortion to be performed in PHC is the abortion within the first trimester, that previous ultrasound imaging is not necessary and that self-management of the procedure at home should be presented as a possibility. With this regard, international guidelines demonstrate that the WHO recommendations may be put into practice in different scenarios, considering the several realities of the countries included in the study.
Lastly, considering the Brazilian context, it is necessary to highlight that both the laws and the regulation of the procedure are retrograde compared to most countries included in this study. In the face of several initiatives for restricting even more the access to legal abortion occurred in the last years, not receding does not seem sufficient; it is necessary to advance in the assurance of this reproductive right in the country. We expect that this article, when assessing international experience of provision of abortion in PHC, may be a subsidy for this advance.
AcknowledgementsWe would like to thank the Graduate Program in Public Health at ENSP/Fiocruz for funding the translation services, through the Academic Excellence Program (CAPES/PROEX).
References1. World Health Organization (WHO). Abortion care guideline. Geneva: WHO; 2022. [access in 2022 Mai 5]. Available from:
https://apps.who.int/iris/handle/10665/34931622. Starfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília (DF): UNESCO, Ministério da Saúde; 2002. [access in 2023 Mai 6]. Available from:
https://unesdoc.unesco.org/ark:/48223/pf00001308053. World Health Organization (WHO). Safe abortion: technical and policy guidance for health systems. 1
st ed. Geneva: WHO; 2003 [acesso em 2022 Mai 05]. 110 p. Available from:
https://apps.who.int/iris/bitstream/handle/10665/42586/9241590343-eng.pdf?4. Presidência da República (BR). Decreto-Lei No 2.848, de 7 de dezembro de 1940. Código Penal. Rio de Janeiro (RJ): DOU de 31 de dezembro de 1940. [access in 2022 Mai 5]. Available from:
http://www.planalto.gov.br/ccivil_03/decreto-lei/del2848compilado.htm5. Supremo Tribunal Federal (BR). Arguição de Descumprimento de Preceito Fundamental 54. Anencefalia. Brasília (DF): 2012. [access in 2022 Mai 5]. Available from:
http://www.stf.jus.br/arquivo/cms/noticianoticiastf/anexo/adpf54.pdf6. Jacobs MG, Boing AC. O que os dados nacionais indicam sobre a oferta e a realização de aborto previsto em lei no Brasil em 2019? Cad Saúde Pública. 2021; 37 (12): e00085321.
7. Jacobs MG, Boing AC. Como a normatização sobre o serviço de aborto em gravidez decorrente de estupro afeta sua oferta nos municípios? Ciênc Saúde Colet. 2022; 27 (9): 3689-700.
8. Ministério da Saúde (BR). Portaria de Consolidação Nº 5, de 28 de setembro de 2017. Consolidação das normas sobre as ações e os serviços de saúde do Sistema Único de Saúde. Brasília (DF): DOU 3 de outubro de 2017. [access in 2022 Mai 5]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2017/prc0005_03_10_2017.html9. World Health Organization (WHO). Global Abortion Policies Database [
Internet]. 2017. [access in 2022 Mai 5]. Available from:
https://abortion-policies.srhr.org/10. Ministério da Saúde (BR). Departamento de Ações Programáticas Estratégicas. Atenção humanizada ao abortamento: norma técnica. 2
nd ed. Brasília (DF): Ministério da Saúde; 2011. [access in 2022 Mai 5]. Available from:
http://bvsms.saude.gov.br/bvs/publicacoes/atencao_humanizada_abortamento_norma_tecnica_2ed.pdf11. National Department of Health (ZA). National Guideline for Implementation of the Choice on Termination of Pregnancy Act. Pretoria: National Departmentof Health; 2019. [access in 2023 Abr 30]. Available from:
https://www.health.gov.za/wp-content/uploads/2023/04/Termination-Pregnancy-Guideline_Final_2021.pdf12. Federal Ministry of Health (ET). Technical and Procedural Guidelines for Safe Abortion Services in Ethiopia (second edition). Addis Ababa: Federal Ministry of Health; 2014. [access in 2023 Abr 1]. Available from:
https://platform.who.int/docs/default-source/mca-documents/policy-documents/guideline/ETH-RH-18-01-GUIDELINE-2014-eng-Safe-Abortion-Services.pdf13. Ministério da Saúde (MZ). Diploma Ministerial n.o 60/2017: Aprova as Normas clínicas sobre Aborto Seguro, Cuidados Pós-Aborto e define as condições em que a interrupção voluntária da gravidez deve ser efectuada nas Unidades Sanitárias do Serviço Nacional. Imprensa Nacional de Moçambique; 2017. [access in 2023 Abr 1]. Available from:
https://www.wlsa.org.mz/wp-content/uploads/2017/11/Diploma_Ministerial_60-2017.pdf14. Ministry of Health (ZM). Zambia Standart Treatment Guideline (5
th edition). Lusaka: Ministry of Health; 2020. [access in 2023 Abr 1]. Available from:
https://www.moh.gov.zm/?wpfb_dl=3215. Ministerio de Salud de la Nación (AR). Protocolo para laatención integral de las personas conderecho a la interrupción voluntaria y legal delembarazo: actualización 2022. 1ª ed. Ciudad Autónoma de Buenos Aires: Ministerio de Salud de la Nación; 2022. [access in 2023 Abr 1]. Available from:
http://bancos.salud.gob.ar/recurso/protocolo-para-la-atencion-integral-de-las-personas-con-derecho-la-interrupcion-voluntaria16. Ministerio de Salud y Protección Social (CO). Atención integral de la interrupción voluntaria delembarazo (IVE) enel primer nivel de complejidad. Documento técnico para prestadores de servicios de salud. Bogotá: Ministerio de Salud y Protección Social; 2014. Available from:
https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/SM-IVE-Atencion-baja-complejidad.pdf17. Secretaría de Salud (MX). Lineamiento técnico para la atención del Aborto Seguro en México. Secretaría de Salud; 2022. [access in 2023 Mai 26]. Available from:
https://www.gob.mx/cms/uploads/attachment/file/779301/V2-FINAL_Interactivo_22NOV_22-Lineamiento_te_cnico_aborto.pdf18. Ministry of Health and Family Welfare (BD). Woman-centered Menstrual Regulation and Postabortion Care Services: Reference manual. 3
rd ed. Dhaka: Ipas Bangladesh; 2021. [access in 2023 Abr 1]. Available from:
https://dgfp.gov.bd/sites/default/files/files/dgfp.portal.gov.bd/miscellaneous_info/9c3b06a2_ff40_4214_a6f5_6cc640abdfa2/2023-08-17-08-05-954637373118126b93f89e3d8cd0ddda.pdf19. Ministry of Health (KH). National protocol Comprehensive Abortion Care. Phnom penh: Ministry of Health; 2010 [access in 2023 Abr 26]. Available from:
https://nmchc.gov.kh/en/national-protocol-comprehensive-abortion-care-2010/20. Ministry of Health and Family Welfare (IN). Comprehensive abortion care: Training and service delivery guidelines. New Delhi: Ministry of Health and Family Welfare; 2018 [access in 2023 Abr 28]. Available from:
https://nhm.gov.in/New_Updates_2018/NHM_Components/RMNCHA/MH/Guidelines/CAC_Training_and_Service_Delivery_Guideline.pdf21. Ministry of Health (SG). Guidelines on termination of pregnancy. Ministry of Health; 2015 [access in 2023 Abr 27]. Available from:
https://www.moh.gov.sg/docs/librariesprovider5/licensing-terms-and-conditions/revised-guidelines-on-termination-of-pregnancy-(dated-17-apr-2015).pdf22. Servicio Canario de la Salud (ES). Protocolo de actuación - Aborto inducido - Comunidad Autónoma de Canarias. Gobierno de Canarias; 2012 [access in 2023 Mai 18]. Available from:
https://www3.gobiernodecanarias.org/sanidad/scs/content/ee23ad48-0327-11e3-8241-7543da9dbb8a/ActuacionAbortoInducido.pdf23. Royal College of Physicians of Ireland. Interim Clinical Guidance: Termination of pregnancy under 12 weeks. Dublin: Institute of Obstetricians & Gynaecologists; 2018 [access in 2023 Abr 1]. Available from:
https://www.hse.ie/eng/about/who/acute-hospitals-division/woman-infants/clinical-guidelines/interim-clinical-guidance-termination -of-pregnancy-under-12-weeks-2018-.pdf24. Assembleia da República (MZ). Lei n.o 24/2019: Lei de Revisão do Código Penal e revoga o artigo 2 do Decreto-Lei n.o 182/74, de 2 de Maio e o Código Penal aprovado pela Lei n.o 35/2014 de 31 de Dezembro. Imprensa Nacional de Moçambique; 2019. [access in 2023 Abr 1]. Available from:
http://www.ts.gov.mz/images/Lei_24-2019_-_Lei_de_Revisao_do_Codigo_Penal_1.pdf25. Corte Constitucional (CO). Comunicado 5: Febrero 21 de 2022. Sentencia C-055-22. Corte Constitucional de Colombia; 2022. [access in 2023 Abr 1]. Disponível em:
https://www.corteconstitucional.gov.co/comunicados/Comunicado%20de%20prensa%20Sentencia%20C-055-22%20-%20Febrero%2021-22.pdf26. Jefaturadel Estado (ES). LeyOrgánica 2/2010, de 3 de marzo, de salud sexual y reproductiva y de lainterrupción voluntaria delembarazo. Madrid: Boletín Oficial del Estado; 2010. [access in 2021 Mai 22]. Available from:
https://www.boe.es/eli/es/lo/2010/03/03/2/con27. Ministerio de Sanidad y Política Social (ES). Real Decreto 831/2010, de 25 de junio, de garantía de la calidad asistencial de la prestación a la interrupción voluntaria del embarazo. Madrid: Boletín Oficial del Estado; 2010. [access in 2023 Jun 15]. Available from:
https://www.boe.es/diario_boe/txt.php?id=BOE-A-2010-1015428. Flick U. Utilização de documentos como dados. In: Flick U. Introdução à pesquisa qualitativa. 3
rd ed. Porto Alegre: Artmed; 2009. p. 230-7
29. Programa das Nações Unidas para o Desenvolvimento (PNUD). Relatório do Desenvolvimento Humano de 2021/2022. Nova Iorque: PNUD; 2022 [access in 2023 Jun 9]. Available from:
https://hdr.undp.org/system/files/documents/global-report-document/hdr2021-22overviewpt1pdf.pdf30. World Health Organization (WHO). Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: World Health Organization; 2023 [access in 2023 Jun 10]. Available from:
https://www.who.int/publications-detail-redirect/978924006875929.31. Taylor L. How South America became a global role model for abortion rights. BMJ. 2022; 378: o1908
32. Goes EF, Ferreira AJF, Meira KC, Myrrha LJD, Reis APD, Nunes VGDA, Santos JMS, Pinto NR, Santos MES, Oliveira HCG, Ramos DO. Desigualdades raciais nas tendências da maternidade adolescente e no acesso ao pré-natal no Brasil, 2008-2019. Res Soc Dev. 2023; 12 (1): e8312139404.
33. World Health Organization (WHO). Web Annex A. World Health Organization Model List of Essential Medicines – 23rd List, 2023. In: The selection and use of essential medicines 2023: Executive summary of the report of the 24th WHO Expert Committee on the Selection and Use of Essential Medicines, 24 – 28 April 2023. Geneva: WHO; 2023. [access in 2024 Jan 2]. Available from:
https://iris.who.int/bitstream/handle/10665/371090/WHO-MHP-HPS-EML-2023.02-eng.pdf?sequence=134. Paro HBMS, Rosas CF. Posicionamento Oficial da Rede Médica pelo Direito de Decidir: Pela manutenção dos serviços de aborto legal no Brasil em tempos de pandemia. 2020 [access in 2023 Jun 11]. Available from:
https://globaldoctorsforchoice.org/wp-content/uploads/Nota-GDC-Covid-19-abortion_Portuguess.pdf.pdf35. Ministério da Saúde (BR). Portaria Nº 2.282, de 27 de agosto de 2020. Dispõe sobre o Procedimento de Justificação e Autorização da Interrupção da Gravidez nos casos previstos em lei, no âmbito do Sistema Único de Saúde-SUS. Brasília (DF): DOU 28 de agosto de 2020. [access in 2023 Jul 11]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2020/prt2282_28_08_2020.html36. Diniz D. Maternal mortality: when a pandemic overlaps with the anti-gender crusade [Editorial]. Dev World Bioeth. 2020; 20 (3): 116-7.
37. Jacobs MG, Boing AC. Travel as a barrier to abortion provided by law access. Brazil, 2010-2019. Rev Bras Saúde Materno Infant. 2022; 22 (4): 853-61.
38. Giugliani C, Ruschel AE, Belomé da Silva MC, Maia MN, Pereira Salvador de Oliveira DO. O direito ao aborto no Brasil e a implicação da Atenção Primária à Saúde. Rev Bras Med Fam Comunidade. 2019; 14 (41): 1791.
39. Murphy C. A Irlanda desde a revogação da Oitava Emenda. Cad Saúde Pública. 2020; 36:e00211119.
40. Horgan P, Thompson M, Harte K, Gee R. Termination of pregnancy services in Irish general practice from January 2019 to June 2019. Contraception. 2021; 104: 502-5.
41. Mishtal J, Reeves K, Chakravarty D, Grimes L, Stifani B, Chavkin W, Duffy D, Favier M, Horgan P, Murphy M, Lavelanet A. Abortion policy implementation in Ireland: Lessons from the community model of care. PLoS ONE. 2022; 17: e0264494.
Author’s contributionMaia MN and Pinto LW: conceptualization, data curation, formal analysis, investigation, methodology, validation, writing and review of the manuscript. All authors approve the final version of the article and declare no conflict of interest.
Received on September 5, 2023
Final version presented on August 3, 2024
Approved on August 14, 2024
Associated Editor: Melânia Amorim


 ; Liana Wernersbach Pinto 2
; Liana Wernersbach Pinto 2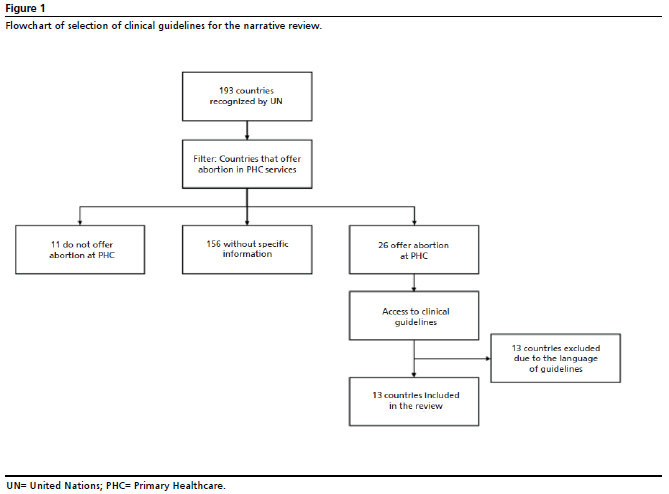






 Ler em português
Ler em português