ABSTRACT
OBJECTIVES: to analyze the geographic distribution of breast cancer care services in Pernambuco, northeastern Brazil.
METHODS: a descriptive cross-sectional study analyzing the geographic distribution of breast cancer care services, which used the National Registry of Health Facilities, State Oncology Plan, and Outpatient and Hospital Information Systems, in 2022. The tools used in the analysis were Excel 2021, TabWinDataSUS, and Geo-clip Dubbed version.
RESULTS: the geographic distribution and care flows revealed regional disparities, especially in macro-regions II, III, and IV. Macro-region I is the best equipped, concentrating the majority of mammograms (64.4%), in addition to having the majority of ultrasound equipment (64.5%) and cancer treatment services (65.1%). The absence of breast biopsy services in the SUS was observed in the National Registry of Health Facilities. Of the seven units indicated in the oncology plan, three did not perform biopsies in the last five years, and two started in 2022.
CONCLUSION: the results highlighted the need for (re)organization of the breast cancer care network and the distribution of health services, considering local needs, through the implementation of the care line with adequate flows, providing timely and equitable care.
Keywords:
Oncology, Breast neoplasms, Access to health services, Equity, Integrality
RESUMO
OBJETIVOS: analisar a distribuição geográfica dos serviços de saúde da linha de cuidado do câncer de mama em Pernambuco, Nordeste do Brasil.
MÉTODOS: estudo descritivo transversal com análise da distribuição geográfica dos serviços da linha de cuidado do câncer de mama, que utilizou o Cadastro Nacional de Estabelecimentos de Saúde, Plano Estadual de Oncologia e Sistemas de Informações Ambulatoriais e Hospitalares, no ano de 2022. As ferramentas empregadas na análise foram o Excel 2021, o TabWin DataSUS e o Geoclip versão Dubded.
RESULTADOS: a distribuição geográfica e os fluxos assistenciais revelaram disparidades regionais, especialmente nas Macrorregiões II, III e IV. A Macrorregião I é a mais equipada, concentrando a maioria dos mamógrafos (64,4%), além de possuir a maioria dos equipamentos de ultrassonografia (64,5%) e serviços de tratamento de câncer (65,1%). Observou-se a ausência de serviços para biópsia de mama no SUS no Cadastro Nacional de Estabelecimentos de Saúde. Das sete unidades indicadas no plano de oncologia, três não realizaram biópsias nos últimos cinco anos, e duas iniciaram em 2022.
CONCLUSÃO: os resultados evidenciaram a necessidade de (re)organizar a rede de atenção ao câncer de mama e a distribuição dos serviços de saúde, considerando necessidades locais, através da implementação da linha de cuidado com fluxos adequados, proporcionando atendimento oportuno e equitativo.
Palavras-chave:
Oncologia, Câncer de mama, Acesso aos serviços de saúde, Equidade, Integralidade
IntroductionBreast cancer is the most common malignant neoplasm within women, standing out as an important public health problem due to its high incidence and mortality. In Brazil, it is the most recurrent tumor, responsible for 15% of new cases of cancer.
1,2 In 2022, 19,103 deaths due to the disease occurred in the country, and the Northeast region was the second in number of deaths, with 4195 cases, of which 832 occurred in Pernambuco.
3 High mortality is associated, mainly, with late diagnosis.
2,4Due to the magnitude of breast cancer, the Unified Health System (SUS – Portuguese acronym) should structure the Healthcare Network (RAS – Portuguese acronym) to ensure promotion, prevention, early diagnosis and adequate treatment. The health promotion includes awareness campaigns, whilst prevention demands access to regular mammogram screening and fast diagnosis.
4,5,6In the SUS, cancer treatment is performed in specialized hospitals: the High Complexity Oncology Units (Unacon – Portuguese acronym), which treat the most common cancers; and the High Complexity Oncology Centers (Cacon – Portuguese acronym), which treat all types of cancer. Besides, there are isolated radiotherapy services. In Pernambuco, there are services that are reference in Oncology in all health macro-regions.
4,7,8,9,10The opportune access to health services plays a crucial role in the prognosis and survival of uses, as well as in costs for the SUS.
4,6,7,8,9,10 The care pathways come as strategic management instruments, integrating the primary, secondary and tertiary healthcare of the RAS.
The incorporation of the integrality principle is essential for the implementation of the care pathway focused on breast cancer in the SUS. In this context, it is indispensable to establish a regionalized offer of these services, ranging both screening and treatment, in order to assure a broad and effective approach for users affected by this condition.
11Integrality encompasses several conceptualizations and dimensions, involving actions and attitudes that expand the comprehension of individual needs. The study aimed in the dimension of integrality, organization of health services and regionalization of units in order to build a healthcare system.
12The process of regionalization has an important resource, which is the health map. The latter allows the mapping and geographic analysis of the distribution of health services offered by both the SUS and private networks.
13 The inequalities of access, infrastructure and operational capability of health services, lack of specialized professionals, geographic barriers and the lack of integration between the different levels of healthcare within the macro-region are challenges for the SUS.
The identification of networks constitutes an essential tool in the planning and improving of the distribution of health services, since the geographic access influences directly the outcomes of treatment. When structuring the service network, is essential to consider both access and accessibility.
14 The geographic accessibility, defined in this study as the physical distance between the facility of provision of healthcare service and the residence of the user, is a crucial component of the access.
14,15The analysis of geographic distribution of health services and assistance flows may reveal regional disparities. This information subside the strategic planning for the care to women with breast cancer, promoting more effective and equitable responses in the Health Macro-regions. The study aimed to describe the geographic distribution of health services in the care pathways of breast cancer in Pernambuco, Northeast of Brazil.
MethodsDescriptive cross-sectional study, which used secondary data available in the National Registry of Health Facilities (CNES – Portuguese acronym), in the State Planning of Oncology of Pernambuco
16 and in the Outpatient Information Systems (SIA/SUS – Portuguese acronym) and Hospital Information Systems (SIH/SUS – Portuguese acronym), in September 2022.
The variables analyzed include the number of mammography equipment, ultrasound, services that perform breast biopsy and breast cancer treatment, besides the number of procedures performed in 2022, for the identification of assistance flows.
The research was carried out in the state of Pernambuco, one of the 27 federative units of Brazil, composed of 184 municipalities and an additional area (Fernando de Noronha Island), the city of Recife as its capital. It is the seventh most populous state in the country, with around 9,058,931 inhabitants, which are 4.6% of the national population, approximately, with a demographic density of 89.5 inhabitants/km
2. In the healthcare area, Pernambuco is divided into fourMacro-regions and 12 health regions: Metropolitan (regions I, II, III and XII), Agreste (IV and V), Sertão (VI, X and XI) and Vale do São Francisco e Araripe (VII, VIII and IX).
12The study used data from the services used for screening, diagnosis and treatment of breast cancer. In order to screen breast cancer, we used the distribution of analog mammogram machines, digital mammogram machines and mammogram machines with stereotactic, as well as conventional and Doppler ultrasound.
For the diagnosis, it was not possible to locate the services that perform breast cancer biopsy in the CNES, and the Specialized Emergency Care Units (UPAE – Portuguese acronym) were identified by the outpatient production of the last five years, which were considered a reference for the procedure in the State Planning of Oncology.
16In the treatment, we used the variable “Facilities that offer oncology service”, characterizing them as “SUS”, “SUS and Private Care” and “Private Care”. As private health, we refer to the assistance provided with private funds (direct payment to the care provider by the user), and by means of health insurance plans.
In order to identify the organizational structure in the health map of each region, for breast cancer, data were systematized per health region and macro-region, considering the Pernambuco Master Plan for Regionalization,
17 observing the geographic distribution and offer of equipment and prioritized services in this care pathway, considering the absolute number of equipment in the states, which were “in use” and “in use in SUS”.
With the information extracted from CNES and the State Oncology Plan, concerning the number of mammogram machines, ultrasound equipment, biopsy services for breast cancer and services that performed breast cancer treatment, we built a database using the Excel 2021 software, including information collected in the 185 municipalities of Pernambuco, in sequence, they were clustered by their respective health regions and macro-regions. The process of analysis was performed with the Excel software, in which data were expressed in charts considering descriptive statistics and variables were described in absolute and relative frequencies. Data were systematized per health macro-region.
For the visual representation of assistance flows, information wasextracted from SIA/SUS and SIH/SUS using the platform TabWin from DataSUS of the Ministry of Health, considering mammograms, breast ultrasounds, biopsies and breast cancer treatment performed in 2022. TabWin was chosen due to its capability of identification of dominant flows, that is, representing those with higher frequency of registered events. This approach was adopted in order to avoid visual pollution in maps, assuring that only the most relevant flows were highlighted.
The results were visualized with two tools of map creation: TabWin, which has geographic information system functions, developed by DataSUS, and the Geoclip software version
dubded, an interactive tool for representation of geographic information. For maps with the availability of equipment, the latter were represented by means of proportional symbols superposed in the polygon of the municipality that houses them, that is, that has them installed. Its diameter represents the quantity of available units for a determinate equipment type, as well as its status: whether they are linked to SUS or not.
The outpatient and hospital production was used to create maps of assistance flow, identifying the origin of users and the location of exams/procedures, indicating whether women are using the services in their own macro-regions.
The present study was approved by the Research Ethics Committee of the Institute of Research Aggeu Magalhães, Certificate of Presentation of Ethic Appraisal 67124722.2.0000.5190.
ResultsIn September 2022, Pernambuco possessed 205 operational mammogram machines. Of these, 59% were being used in the SUS (owned under contracts). Concerning the type and quantity of operational mammogram machines in the state, we observed that 66.3% are analog, 20.5% are digital and 13.2% have stereotactic, as shown in Table 1.
The results of Table 1 reveal that the Macro-region I has most of the mammogram machines of the state (64.4%) and 53% are being used in SUS. The region I also concentrates most of mammogram machines with stereotactic (74.1%), with emphasis in Recife, which possesses 44.4% of the devices with this technology that are operating in the state. The macro-regions I, III and IV have 35.6% of the devices in operation, the two latter with less quantity and variety of equipment.
With regard to ultrasound, of the 1280 equipment in use in the state, 47.5% have Doppler. Also on this topic, the Macro-region I concentrates the equipment, with 64.5% of the total, of which 71.2% have Doppler. In sequence, the macro-regions II, III and IV, with 35.5% of equipment. It draws attention to the scarcity in macro-regions III and IV, as shown in Table 1.
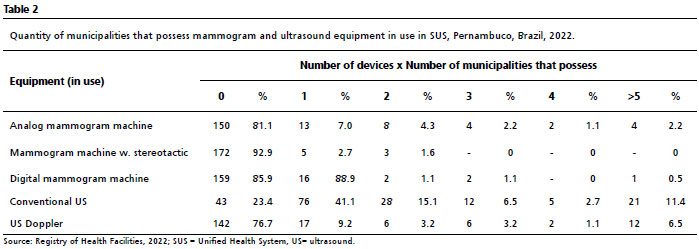
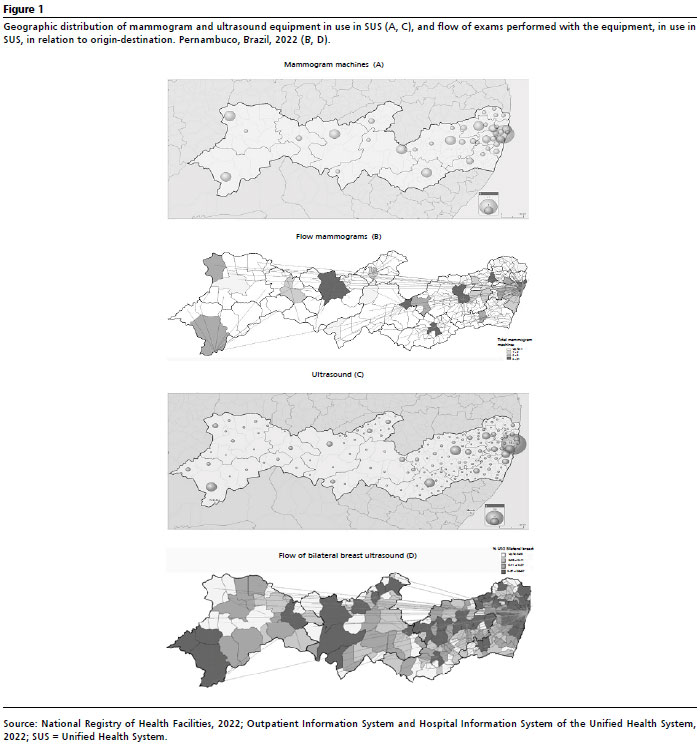
Analyzing the distribution by municipalities, 77.3% do not possess mammogram machines in use in the SUS, whilst only 2.2% have more than four devices. In the case of ultrasound, 18.9% of municipalities do not possess any equipment, and most do not have equipment with Doppler (76.8%) or those conventional (23.2%), according to Table 2 and Figure 1, which show the spatial distribution of mammogram machines and ultrasound equipment in use in the SUS, according to health region, Macro-region and assistance flows.
The State Oncology Plan has seven UPAE, of medium complexity, for breast cancer diagnosis. In Macro-region I, UPAE Limoeiro, Great Recife and Goiana; in Macro-region II, UPAE Caruaru and Garanhuns; in Macro-region III, UPAE Arcoverde and in Macro-region IV, UPAE Petrolina.
There was no registry of biopsies in the UPAEs in Limoeiro, Great Recife and Goiana in the last five years. The UPAE Caruaru did not perform biopsies in 2019, performed 16 in 2020, 98 in 2021 and 107 in 2022. The UPAE Garanhuns, during the same period, had ten registries of biopsies, all in 2022. The UPAE Arcoverde did not perform any biopsy in 2019, performed 32 in 2020, 32 in 2021 and 113 in 2022. The UPAE Petrolina performed 32 biopsies in 2022, without registry of previous years.
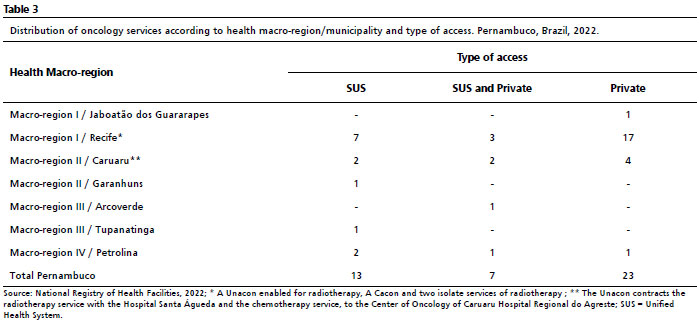
Pernambuco possesses 43 services that perform breast cancer treatment, 30.2% exclusively by SUS, 16.3% mixed (SUS and private) and 53.5% only private. The Macro-region I concentrates 65.1% of these services, with 25% attending exclusively by SUS, 10.7% mixed and 64.3% only private (Table 3).
The Macro-region I also leads in hospitals specialized in oncology, with 55.5% of the total of the state, including four Unacon units and one Cacon unit, besides two radiotherapy services in Recife. Macro-region II represents 20.9%, with nine facilities specialized in oncology, 33.3% exclusively by SUS, 22.2% mixed and 44.5% only private (Table 3).
The Macro-region III has 4.7% of the facilities with oncology service, one exclusively by SUS and one mixed (SUS and private) in the city of Arcoverde. The Macro-region IV possesses 9.3%, two exclusively by SUS, one mixed and only one private. One of the four services of the Macro-region IV is the Unacon in Petrolina, of the health region VIII (Table 3).
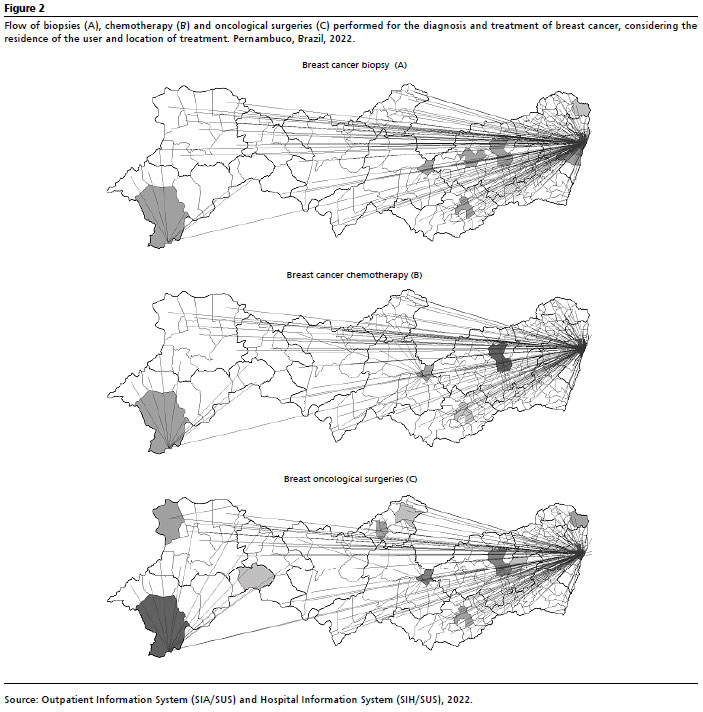
Figure 2 presents the spatial distribution of services that performed biopsies and treatment of breast cancer, highlighting the assistance flows of Macro-regions I, II, II and IV. Data reveal a significant concentration in Macro-region I, with few flows in the other macro-regions and the migration of users to perform biopsies and treatment in Macro-region I, certainly due to the concentration of services in this macro-region.
Concerning the assistance flows for chemotherapy and oncologic surgery, there was a significant concentration in Macro-region I, with few registries of the other regions and the displacement of users to Macro-region I (Figure 2).
DiscussionThe geographical analysis found regional inequalities in the availability and use of services of screening, diagnosis and treatment of breast cancer in the macro-regions. The manner by which the services are organized may affect the access of women within their own macro-regions. We highlight the importance of considering the role of regional references and the interaction between municipalities in the health regions. The assistance flows reveal potential weaknesses in the agreement between the regions, with the migration of users of macro-regions II, III and IV to macro-region I in all analyzed services.
The opportune access to oncology services is a challenge for the management of all health regions, mainly with regard to the access to pathological diagnosis services, which is insufficient in the SUS network of the state of Pernambuco, and there is no database available in order to guide professionals and users for this type of service. Women that depend exclusively on the public healthcare network face greater barriers to perform the mammogram screening.
4,18,19The concentration of services in the health region I of the Macro-region I may be one of the main factors that have impaired the expansion of access to services of the Care Pathway of the state of Pernambuco, since the distribution of equipment in use in SUS is unequal in the Health Macro-regions II, III and IV.
18 The scarcity of equipment possibly means that some women never performed screening exams.
18,20We highlight, thus, the necessity of (re)organization of services and referrals between municipalities and health regions, since the analyzed flows demonstrated several municipalities exceeding the limits of the regions and macro-regions of origin.
The migration of women to other municipalities, even when there are mammogram machines and ultrasound equipment available locally, evidence problems in the territorial logistics and efficacy of regionalization. Although macro-region I concentrates more ultrasound equipment due to its population, the inequality in the offer of these services in macro-regions II, III and IV lead to the migration to areas with more assistance, revealing gaps in the planning and regional management of health, which demand concrete actions to improve the regionalization and communication.
12,18,21The fragmentation of the care pathway is evident, with scarcity of services of reference for breast cancer in the macro-regions II, III and IV in all analyzed services, concerning services of biopsy, it is perceived in the four analyzed macro-regions. The production of the UPAEs over the five years shows the need for strengthening of the structure and organization of the offer of diagnosis exam in the state network. A study about breast cancer screening in Brazil revealed concerns with the access to diagnosis, highlighting the low proportion of diagnosis procedures compared to estimates. Moreover, it identified inequalities in the offer and use of these procedures between the different Brazilian regions.
22The time of diagnosis and opportune access to treatment are compromised, since SUS do not have sufficient service in all health macro-regions to meet the local demands or they are not well distributed, with flow designs and protocols of access of the State Oncology Plan, considering the geographic characteristics of territory, the location of the user, the nearest service, the waiting period and socioeconomic profile, so that it can assure the compliance with laws of 30 and 60 days.
23,24With regard to diagnosis, the results show the need for Specialized Care of the Ministry of Health, together with the states, in order to expand the offer of diagnosis in a global perspective, structuring the already existing services and implementing newer. We infer that one of the possible impairments in the increase of agreements with pathology laboratories is due to the costs established in the table of procedures of SUS, which do not reach the operational cost of exams.
25Although the macro-regions I, II, III and IV possess Unacon, the access to treatment requires confirmed cancer diagnosis in seven of them, and/or imaging with BI-RADS (Breast Image Reporting and Data System) 4 or 5, in two services.
26The assistance flow of breast cancer biopsies do not corroborate the services presented in the State Oncology Plan. Besides the geographic barrier to the execution, the users have been dealing with the organizational barrier of service distribution, and consequently, there are situations in which women need to rely on private service diagnosis on their own, in order to optimize the treatment. Women followed-up in public services, compared to those in private services with health insurance have worse prognosis and die early compared to women with the disease and possess such insurance.
4,27The difficulty in accessing cancer treatment services may lead to the following consequences: inadequate treatment, unfavorable prognoses and decrease of user’s quality of life.
15 The results of the study indicated that municipalities that are part of the macro-region I, specifically the health region I, also concentrate the highest part of services for breast cancer treatment, and are responsible for the execution of the highest demand for services of the municipalities of the four health macro-regions of the state. A study carried out in Pernambuco identified the evasion of users from the countryside to have treatment in the capital.
26The structural differences, availability of professionals and protocols of access have leading to the evasion of women of the countryside to the capital of the state, including municipalities that possess Unacon.
26The treatment of breast cancer is not regulated in the state of Pernambuco.
26This leads to problems that impair the quality and efficacy of care, including inequality in the access to services present in the macro-regions, lack of standardization of protocols, difficulties in the coordination of care and fragmentation of assistance. The regulation plays a crucial role when it establishes mechanisms for the management and assessment of performance of services, displacement of women with breast cancer, which are essential to ensure the opportune access to services.
14 Previous studies highlighted the large distances traveled by users to hospitals that offer oncologic services in Brazil.
14,15,26.28,29There is evidence that late treatments are related to regional inequalities.
15,26,30 The increase in the demand for displacement of users with cancer has been associated with advanced stages of the disease in the moment of diagnosis, inadequate treatment, unfavorable prognosis and an inferior quality of life.
30 Therefore, in the countryside, there is still the challenge of implementing new services and restructuring the already existent, in order to ensure not only the presence of the service, but its functionality.
26When analyzing the lack of assistance in some regions and the long displacements of users to other areas, we highlight the urgency of investments and care in the regions that lack services and equipment. Although there are 43 services for cancer treatment in Pernambuco, most are located in the supplementary healthcare, concentrating mainly in the Macro-region I. The telehealth may be an essential tool for expanding the access,
16 reduce costs with Treatment Out of Household and improve the quality of assistance, mainly in areas with distance barriers, such as the Macro-region IV of the state of Pernambuco, where women perform long travels for treatment in Macro-region I.
15,16,26It is important to consider the limitations of this study. The main limitation is related to the CNES database, which does not possess enough information on the location of services related to SUS for pathological diagnosis. This impaired the assessment of the quantity of services offered. Moreover, the State Oncology Plan mentions only the UPAEs, which also limits the analysis.
The study reveals significant disparities in the availability of services of screening, diagnosis and treatment of breast cancer in the different macro-regions of Pernambuco. The concentration of services in the macro-region I limits the availability of assistance in other macro-regions, emphasizing the access inequalities for women.
We conclude that it is essential to organize the healthcare services and the specific demands of each macro-region in order to ensure integrative and universal access. We recommend the implementation of care pathways, permanent qualification of professionals, development of personalized approaches and review of the current health map. Moreover, it is necessary to enhance the management and updating of CNES and promote further studies about access and quality of services.
References1. Instituto Nacional do Câncer (INCA). Estimativa 2023: incidência de câncer no Brasil. [Internet]. Rio de Janeiro: INCA; 2022. [access in 2023 Fev 11]. Available from:
https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/estimativa-2023.pdf2. Santos MO, Lima FCS, Martins LFL, Oliveira JFP, Almeida LM, Cancela MC. Estimativa de Incidência de Câncer no Brasil, 2023-2025. Rev Bras Cancerol. 2023 69 (1): e213700.
3. Ministério da Saúde (BR). Óbitos p/Residência segundo Região/Unidade da Federação. Grupo CID-10: Neoplasias malignas da mama. [
Internet]. Brasília (DF): Ministério da Saúde; 2023. [access in 2024 Abr 6]. Available from:
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/obt10uf.def4. Silva GA, Souza-Júnior PRB, Damacena GN, Szwarcwald Cl. Early detection of breast cancer in Brazil: data from the national health survey, 2013. Rev Saúde Pública. 2017; 51(1): 14.
5. Horton S, Rodriguez RC, Anderson BO, Aung S, Awuah B, Pebé LD,
et al. Health system strengthening: integration of breast cancer care for improved outcomes. Cancer. 2020; 126 (10): 2353-64.
6. Ginsburg O, Yip C, Brooks A, Cabanes A, Caleffi M, Yataco JAD,
et al. Breast cancer early detection: a phased approach to implementation. Cancer. 2020; 126 (10): 2379-93.
7. Sousa SMMT, Carvalho MGFM, Santos Júnior LA, Mariano SBC. Acesso ao tratamento da mulher com câncer de mama. Saúde debate. 2019; 43 (122): 727-41.
8. Vrdoljak E, Balja MP, Marułić Z, Avirović M, Blažičević V, Tomasović Č,
et al. Covid-19 Pandemic Effects on Breast Cancer Diagnosis in Croatia: a population- and registry-based study. Oncologist. 2021; 26 (7): e1156-60.
9. Lana AP, Perelman J, Andrade ELG, Acðrcio F, Guerra AA, Cherchiglia ML. Cost Analysis of Cancer in Brazil: a population-based study of patients treated by public health system from 2001-2015. Value Health Reg Issues. 2020; 23 (137):137-47.
10. Alcântara RG, Milagres CM, Santana SP. Jornada da paciente e levantamento dos custos do acompanhamento do câncer de mama inicial e metastático no Sistema Único de Saúde (SUS). J Bras Econ Saúde. 2022; 14 (1): 51-5.
11. Landim ELAS, Guimarães MCL, Pereira APCM. Rede de Atenção à Saúde: integração sistêmica sob a perspectiva da macrogestão. Saúde Debate. 2019; 43 (5): 161-73.
12. Starfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília (DF): Ministério da Saúde; 2002. [access in 2023 Abr 12]. Available from:
https://unesdoc.unesco.org/ark:/48223/pf000013080513. Brasil. Decreto n° 7.508, de 28 de junho de 2011. Regulamenta a Lei no 8.080, de 19 de setembro de 1990, para dispor sobre a organização do Sistema Único de Saúde - SUS, o planejamento da saúde, a assistência à saúde e a articulação interfederativa, e dá outras providências. Brasília (DF): DOU de 29 de junho de 2011. . [
Internet]. [access in 2023 Abr 12]. Available from:
https://www.planalto.gov.br/ccivil_03/_Ato2011-2014/2011/Decreto/D7508.htm?msclkid=af8d8426d12111ec969c7954231d6d5a14. Travassos C, Martins M. Uma revisão sobre os conceitos de acesso e utilização de serviços de saúde. Cad Saúde Pública. 2004, 20: 190-8.
15. Fonseca BP, Albuquerque PC, Saldanha RF, Zicker F. Geographic accessibility to cancer treatment in Brazil: a network analysis. Lancet Reg Health Am. 2021, 7: 100153.
16. Pernambuco. Plano estadual de oncologia. 2023. [
Internet]. Pernambuco: Secretaria Estadual de Saúde, 2023. [access in 2023 Abr 12]. Available from:
http://portal-antigo.saude.pe.gov.br/sites/portal.saude.pe.gov.br/files/plano_9096744_plano_de_oncologia_.pdf17. Pernambuco. Secretaria Estadual de Saúde. Plano Diretor de Regionalização; 2011. [access in 2023 Abr 12]. Available from:
https://portal-antigo.saude.pe.gov.br/sites/portal.saude.pe.gov.br/files/pdrconass-versao_final1.doc_ao_conass_em_jan_2012.pdf18. Silva MTA, Silva-Júnior VB, Mangueira JO, Gurgel Junior GD, Leal EMM. Distribution of mammograms and mammography offering in relation to the parametric care of the Public Health Care System in Pernambuco. Rev Bras Saúde Matern Infant. 2018; 18 (3): 609-18.
19. Lourenço TS, Mauad EC, Vieira RAC. Barreiras no rastreamento do câncer de mama e o papel da enfermagem: revisão integrativa. Rev Bras Enferm. 2013; 66 (4): 585-91.
20. Rocha ASS, Manfron APT, Franca BHS. Iniquidade socioeconômica na distribuição de equipamentos de imagem na saúde pública brasileira. Rev Latinoam Bioet. 2020; 19 (37-2): 19-27.
21. Almeida MMM, Almeida PF, Melo EA. Regulação assistencial ou cada um por si? Lições a partir da detecção precoce do câncer de mama em redes regionalizadas do Sistema Único de Saúde (SUS). Interface. 2020; 24 (1):1-16.
22. Tomazelli JG, Silva GA. Breast cancer screening in Brazil: an assessment of supply and use of Brazilian National Health System health care network for the period 2010-2012. Epidemiol Serv Saúde. 2017; 26: 713-24.
23. Ministério da Saúde (BR). Lei nº 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Brasília (DF): DOU de 23 de novembro de 2012. [
Internet]. [access in 2023 Abr 12]. Available from:
https://legislacao.presidencia.gov.br/atos/?tipo=LEI&numero=12732&ano=2012&ato=276cXUq1kMVpWT8c524. Brasil. Lei nº 13.896, de 30 de outubro de 2019. Altera a Lei nº 12.732, de 22 de novembro de 2012, para que os exames relacionados ao diagnóstico de neoplasia maligna sejam realizados no prazo de 30 (trinta) dias, no caso em que especifica. Brasília (DF): DOU de 31 de outubro de 2019. [
Internet]. [access in 2023 Abr 12]. Available from:
https://www.planalto.gov.br/ccivil_03/_ato2019-2022/2019/lei/l13896.htm25. Brasil. Portaria Nº 2.730/GM/MS, de 19 de outubro de 2017 - Altera valor e atributos de procedimentos diagnósticos de câncer de mama na Tabela de Procedimentos, Medicamentos, Órteses, Próteses e Materiais Especiais do Sistema Único de Saúde (SUS). Brasília (DF): DOU de 19 de outubro de 2017. [
Internet]. [access in 2023 Abr 12]. Available from:
https://bvsms.saude.gov.br/bvs/saudelegis/gm/2017/prt2730_20_10_2017.html26. Silva RR, Freese de Carvalho EM, Lyra TM, Machado AS. Análise da regulação assistencial na atenção oncológica de alta complexidade em um estado da região Nordeste do Brasil: o câncer de mama como condição traçadora. In: Zarili TF, org. Da prevenção à intervenção: abordagens na saúde coletiva. 2ª ed. Ponta Grossa (PR): Atena Editora; 2024. p. 18-35.
27. Guerra MR, SILVA GA, Nogueira MC, Leite ICG, Oliveira RVC, Cintra JRD,
et al. Sobrevida por câncer de mama e iniquidade em saúde. Cad Saúde Pública. 2015; 31 (8): 1673-84.
28. Saldanha RF, Xavier DR, Carnavalli KM, Lerner K, Barcellos C. Estudo de análise de rede do fluxo de pacientes de câncer de mama no Brasil entre 2014 e 2016. Cad Saúde Pública. 2019; 35 (7): 1-14.
29. Grabois MF, Oliveira EXG, Sa Carvalho M, Grabois MF, Oliveira EXG, Sa Carvalho M. Assistencia ao cancer entre criancas e adolescentes: mapeamento dos fluxos origem-destino no Brasil. Rev Saúde Pública. 2013; 47 (2): 368-78.
30. Nogueira MC, Atty ATM, Tomazelli J, Jardim BC, Bustamante-Teixeira MT, Gulnar A. Frequency and factors associated with delay in breast cancer treatment in Brazil, according to data from the Oncology Panel, 2019-2020. Epidemiol Serv Saúde. 2023; 32 (1): e2022563.
Authors’ contributionSilva RR: planning of research, data survey and collection, discussion of results, writing and final evaluation of the manuscript. Silva IEP: contributed to data collection, presentation of results, discussion of results and final evaluation of the manuscript. Guilhermino GMS: contributed to data collection, review and final evaluation of the manuscript. Velasco WD: contributed to data collection, methodology, presentation of results and final evaluation of the manuscript. Pereira ICAL: contributed to the critical analysis of results and final evaluation of the manuscript. Lyra TM: supervision of the thesis project, review of the work planning, critical analysis of the writing and final review of the manuscript. All authors approve the final version of the article and declare no conflicts of interest.
Received on April 11, 2024
Final version presented on September 10, 2024
Approved on September 12, 2024
Associated Editor: Sheyla Costa


 ; Iris Edná Pereira da Silva 2
; Iris Edná Pereira da Silva 2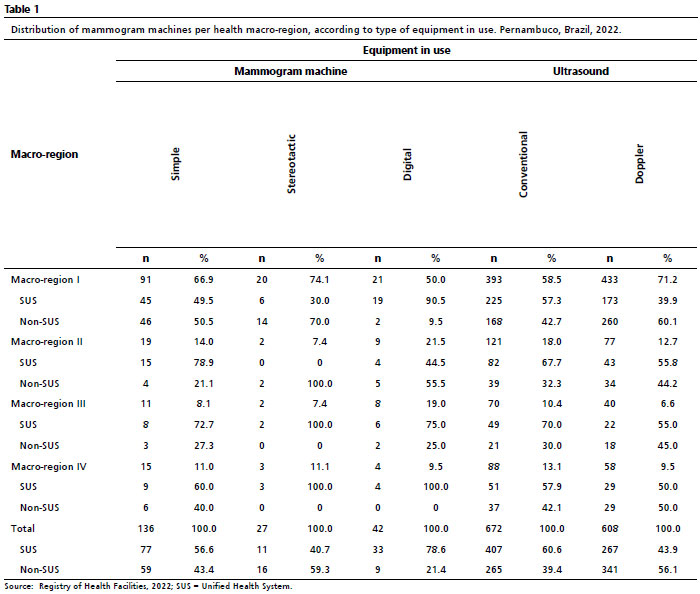






 Ler em português
Ler em português